KEYWORDS
HCV, chronic hepatitis C, elimination, retrieval
BACKGROUND
Chronic hepatitis C virus (HCV) infection targets the liver and, if left untreated, may lead to liver-related complications such as fibrosis, cirrhosis, hepatocellular carcinoma and ultimately death (liver and non-liver related). In 2015, an estimated 71 million people were living with chronic HCV globally and approximately 400,000 people died as a result of the infection.1 For many years, pegylated interferon as combination therapy with ribavirin was standard therapy. Cure rates were low (40-60%) and adverse effects were serious and occurred in many patients. The discovery and development of direct acting antivirals (DAAs) has led to new perspectives as HCV infection can be completely eradicated in the majority of patients with a treatment period of 8 to 12 weeks. Curing HCV infection leads to drastically lower mortality rates even in patients with advanced liver disease.2 In 2016, the World Health Organization (WHO) adopted viral hepatitis elimination targets, aiming for a 90% reduction in new infections, and 65% reduction in mortality by 2030.3 The WHO calls for action in five separate service domains: 1) presence of an up-to-date registration system with accurate data, 2) better testing and quicker access to treatment, 3) engagement of public health, 4) health coverage that is in line with this vision, and 5) innovation in the diagnostic and therapy pipeline. In the Netherlands, these conditions are partially met, which suggests that with targeted effort it is possible to envision a drastic reduction of HCV prevalence and possibly nationwide elimination within a decade. The current paper illustrates the situation of the HCV epidemic in the Netherlands and highlights the targeted efforts that have been taken, thereby reducing HCV-associated morbidity and mortality.
HCV IN THE NETHERLANDS
Historical aspects of the Dutch HCV epidemic
The worldwide epidemic of chronic HCV dates from the 1940s and is probably the result of nosocomial and iatrogenic factors, such as transfusion of HCV-infected blood and blood products and use of unsafe medical equipment.4 These factors similarly fuelled the Dutch epidemic with an estimated 37% of the 1120 haemophilia patients testing HCV positive by the time HCV testing of blood products was introduced in 1992.5 Another key contributor to the Dutch HCV epidemic is risk behaviour such as injection drug use and high risk sex, which was popular during the infamous “flower power” period in the 1960s and 70s. In the Netherlands, this wave of intravenous heroin use created a cohort of 30,000 heroin users in the early 1980s. Two political measures were highly efficient in reducing the risks of heroin use: wide availability and accessibility of opioid substitution therapy such as methadone, and the use of sterile injection equipment as a result of needle exchange programs. By the beginning of the 21st century, hazardous intravenous drug abuse had largely vanished, and along with it a major contributor of the HCV epidemic.6,7 Injection drug use is still unpopular in the Netherlands, which is different from the situation in many other countries, including Europe.8 Male-male sexual contact continues to be the most common mode of transmission in the Netherlands during the last decade.9 Since 2000, sexually transmitted HCV infection outbreaks have been regularly reported in the Netherlands among HIV-infected men who have sex with men (MSM). These outbreaks are currently ongoing, although absolute numbers remain small.10 Finally, HCV is also introduced into the country by first-generation migrants from HCV-endemic countries.
Overall, the HCV epidemic has led to excess mortality. Between 2002 and 2015, around 320 patients died annually due to HCV.11
The Netherlands: the ideal battleground for HCV elimination
The prevalence of HCV in the Netherlands is relatively low (0.16% in 2016),5 compared to other European countries such as France (0.8%), Germany (0.4%), Italy (5.9%) and Romania (3.2%).12 Based on data derived from major relevant risk groups, the number of Dutch chronic HCV carriers in 2016 was estimated at 23,000 people (8,461 – 37,809).5 Group size estimates suggest that first-generation migrants from HCV-endemic countries account for more than half of all HCV-positive persons in the Netherlands (n = 13,819), followed by people who inject or have injected) drugs (PWID, n = 3,131), HIV-positive PWID (n = 303), HIV-positive MSM (n = 672), remaining HIV-positive patients (n = 327), haemophilia patients (n = 423), and individuals at low risk for infection (n = 4,210).5 The absence of nosocomial transmission and controlled injection drug use has led to a very low incidence of acute HCV infections with a reported incidence rate of 0.26 infections per 100,000 in 2016.9 This has resulted in a stationary HCV-infected population of a manageable size. It is likely that if this population is systematically targeted and treated, this will result in a decrease and eventual disappearance of HCV in the Netherlands. Arguments in favour of this may stem from a study that modelled HCV in the Netherlands.13 Researchers tested various disease progression models to predict the future disease burden of HCV in the Netherlands. The study showed that the best and most realistic model of curtailing the HCV epidemic was the ‘increased efficacy and treatment uptake’ scenario, in which sustained virologic responses (SVR) were higher compared to those with the standard treatment regimen of that time (pegylated interferon/ribavirin) and in which a phased increase of treatment uptake was calculated based upon genotype and fibrosis stage. This strategy not only decreases the number of viraemic HCV patients in 2030 by 85%, but also decreases the number of liver-related deaths and hepatocellular carcinoma by 65% and 67%, respectively. These numbers are aligned with the WHO goals for 2030.3 Obstacles in implementing this strategy in order to reduce prevalence of HCV and its complications include the high cost of DAAs and the lack of screening of risk groups for unidentified cases.
The first obstacle, high treatment cost, does not apply to HCV patients in the Netherlands due to the universal insurance system. The Netherlands has a compulsory and comprehensive insurance system with universal coverage regardless of income, age, or employment status. Health insurance providers are legally required to provide a standard benefits package including care provided by general practitioners, hospitals and specialists, and prescription drugs without additional payment. This includes healthcare for chronic hepatitis patients in the 47 dedicated Dutch hepatitis centres, which is fully reimbursed with the exception of the standard non-refundable first payment of € 385.00 for all patients. Since 2015, all European Medicines Agency (EMA)-approved DAAs are available and are fully reimbursed for all HCV genotypes, independent of fibrosis stage, mode of transmission, or comorbidity. The new DAAs yield higher SVR rates than pegylated interferon/ ribavirin combination therapy and they are generally much better tolerated, as is confirmed in real-world settings.14-17 Even genotype 3 patients, previously considered to be difficult-to-treat patients, reach SVR in the majority of cases.18 Since DAA costs became eligible for reimbursment in the Netherlands, an estimated 2,700 patients have been treated in the first year alone.19 It has been estimated that more than 5,000 patients to date, have received DAA treatment. This exceeds the estimates of the model previously-mentioned and means that the current pool of chronic HCV carriers has been reduced from 23,000 to an estimated 18,000 people. This makes the Netherlands an ideal candidate for reaching the WHO viral hepatitis goals well before 2030.
National Hepatitis Plan
In order to achieve the goal of controlling and eliminating the HCV epidemic, the Dutch National Institute of Public Health and Environment (RIVM, Rijksinstituut voor Volksgezondheid en Milieu) has facilitated the development of a National Hepatitis Plan. This plan describes a strategy to control both the hepatitis B virus (HBV) and HCV epidemics and focuses on five areas or pillars: 1) awareness and vaccination, 2) identification of infected patients, 3) diagnosis and treatment, 4) improved organization of hepatitis care, and 5) surveillance systems. The National Hepatitis Plan may be viewed as the Dutch practical translation of the WHO goal towards elimination of viral hepatitis by 2030. The National Hepatitis Plan is endorsed by all relevant stakeholders in the field, including leading HCV experts in the Netherlands, representatives of the Dutch liver patient association (NLV, Nederlandse Leverpatiënten Verening) and the pharmaceutical industry
Strategy for elimination
The first step in HCV elimination is treating as many patients as possible, a paradigm called ‘treatment as prevention’. Two types of approaches seem feasible. First, identification of novel, unidentified cases as a result of screening specific risk groups and of active case finding by general practitioners (GP). Second, re-evaluation (retrieval) of patients with chronic HCV who have been cared for in the past but were lost to follow-up before they were cured. We will discuss both options below.
Screening
Screening strategies designed to eliminate HCV, depending on local prevalence and cost-effectiveness, can either be adopted as a national population screening program or can be used to specifically target high risk populations. The Dutch National Health Council concluded in 2016 that a population-based screening program is not feasible in the Netherlands in view of the relatively low prevalence of HCV and the fact that the majority of infected people will not develop symptoms as a result of the infection. The Council is in favour of case finding in risk populations (such as former and current PWID or migrants) and argues that identification of these cases is the responsibility of related healthcare, such as Community Health Services (GGD, Gemeentelijke Gezondheidsdienst), addiction centres, and prisons. Lastly, the Council recommended screening of HCV among healthcare workers.20 The Minister of Health endorsed these recommendations for risk-based HCV testing as part of an overall strategy to prevent and control HCV infection and HCV-related disease.
Retrieval
Retrieval is the process of tracing patients through the assessment of medical records who have been previously diagnosed with HCV but were somehow lost to follow-up in the following years. These patients are either untreated (for instance, due to contraindications for pegylated interferon) or have been treated but not cured. There are also patients who tested positive for HCV but were not properly linked to care. The loss of follow-up from outpatient clinics of HCV patients who underwent liver biopsy during baseline evaluation has been estimated at 12% after three years,21 and other studies showed a staggering 30% loss to follow-up among patients with HCV at tertiary care centres.22,23 A number of reasons have been suggested for loss to follow-up, such as unawareness of follow-up appointments, or insufficient knowledge of the disease severity and treatment benefit. Prior to 2015, the standard of care for chronic HCV consisted of pegylated interferon combined with ribavirin. The expected side effects stopped many patients from starting therapy and in most cases were lost to follow-up.24 The superior efficiency and safety profile of DAA treatment offers patients a new perspective: cure of chronic HCV without loss of quality of life.25 The introduction of DAAs is the key development that spurred the initiation of HCV retrieval projects, which require cooperation between the primary care, secondary care, tertiary care, and public healthcare.
Several retrieval projects in the Netherlands have been executed. GGD are municipal health organizations for preventive healthcare among the general populations (such as vaccination campaigns) and among certain risk groups for diseases or infections. Several regional GGDs have executed retrieval projects, which identified some lost-to-follow-up HCV patients. However, hospital-based initiatives achieved a larger yield by screening medical records. For example, the “Chronic Hepatitis B and C Recall Northern Holland” aimed to retrieve lost-to-followup patients diagnosed with HVB and HVC between 2001 and 2016 by using data files of the public health system and microbiology laboratories. This approach identified 499 HCV-positive patients and registered 150/499 (30.1%) as lost-to-follow-up. Unfortunately, 126 patients (84%) were not eligible for retrieval due to unknown primary healthcare physicians, unknown home addresses, imprisonment, or relocation to a different region. Four of the 24 retrievable patients were evaluated at the outpatient clinic, resulting in a change of management in 3/4 (75%).23 A general practitioner-based retrieval project in the region of Groningen-Drenthe included patients who tested hepatitis B surface antigen or anti-HCV-positive between 2003 and 2013 but were never referred to a hospital. This project yielded 515 patients, of whom 162 were HCV-positive. Ninety-three (57%) had false-positive HCV test results, died, or could not be traced. Twenty-five of the remaining 77 patients had a current indication for referral, of which 18 (72%) were actually referred to a hepatitis centre.26 The larger “REtrieval And Cure of chronic Hepatitis C patients in the Utrecht region” (REACH) initiative detected HCV patients through screening of HCV-positive test results between 2001 and 2015. This project screened 2,487 HCV patients and filtering led to 269 patients (14.1% of total chronic HCV population in this region) who were eligible for retrieval and invited for screening. So far, 47/269 (17.4%) have visited the outpatient clinic.27 Lastly, a retrieval project executed in the region of Nijmegen-Den Bosch (the Track Trace Treat project) also detected HCV patients through screening of HCV-positive test results between 2003 and 2017. So far, this project has resulted in identification of 175 HCV-positive patients of whom 81 (46%) were lost to follow-up. This study is still ongoing.
Treatment as prevention
In the interferon era, screening and retrieval were not regularly executed, since treatment was not promising due to side effects and suboptimal efficacy. However, treatment with novel DAAs gives screening and retrieval an entirely new ethical line of reasoning. Especially in lost-to-followup patients, caregivers have a certain ethical obligation to retrieve their patients to make them aware of the improved treatment options.
Besides preventing HCV complications, HCV treatment can limit further transmission. Two examples show that a systematic and targeted approach using treatment as prevention will reduce the HCV disease burden. A nationwide elimination program using DAAs in Iceland (TraP Hep C) suggests that treatment is a vital step in national elimination. In Iceland, the prevalence of chronic HCV is 0.3% (estimated 800-1,000 patients in a population of 330,000) and 15 months after launching the program, 479 patients had been evaluated, comprising 48-60% of the estimated total number of viraemic patients. At the time of writing, SVR rates were 96% in 188 of the 292 patients who had finished DAA therapy, and elimination of HCV from Iceland looks like a realistic prospect.28 The second example is the ATHENA effort, which collects Dutch nationwide data from 98% of HIV-infected patients receiving care since 1998. The database contains 23,574 HIV-infected patients who have ever been linked to care, and 1,471 HCV/ HIV co-infected patients (69% MSM, 15% PWID, and 15% unknown HIV transmission route). HCV treatment initiated between 2000 and 2017 reached 1,284 patients (87%), of which 1,124 (76%) were cured. In 6% (92/1471), DAA treatment results are pending.29 When comparing incidence of acute HCV infections in the HIV-positive MSM part of this cohort before and after unrestricted access to DAAs, researchers found a 51% decrease.30 These real-world data are consistent with the concept that HCV “treatment as prevention” averts new HCV infections in a population at risk for acute HCV infections.
HepNed and CELINE
HepNed is a Dutch research foundation supported by the Dutch Society of Hepatology that that is a collaboration between healthcare professionals who provide care for patients with viral hepatitis. As such, it is a consortium of gastroenterologists-hepatologists, internistsinfectious disease specialists, hospital pharmacists, and microbiologists from all eight Dutch University Medical Centres. HepNed is the operational branch that coordinates patient-related viral hepatitis research in the Netherlands. The efforts of HepNed have led to joint studies demonstrating the added value of this collaboration.31
In view of the WHO viral hepatitis elimination targets, recent international developments, and encouraging pilot projects, HepNed designed a strategy that facilitates a nationwide retrieval project: “Hepatitis C Elimination in the Netherlands” (CELINE). CELINE aims to tackle the HCV problem by identifying lost to follow-up chronic HCV patients and giving them appropriate care according to the latest evidence-based guidelines (the online-only available Dutch HCV guidelines32 and/or European Association for the Study of Liver (EASL) Recommendations33). It is a three-year program which started in 2018. CELINE is financially supported through the HCV SCALE program (Screening Access and Linkage to CarE ) from Gilead Sciences.
Structure of CELINE
The CELINE steering committee ensures successful delivery of the project, which include maximizing benefits, monitoring business and strategic issues, and providing advice for the project teams on issues that may endanger the project or impact project rationale or success. The Advisory Board is made up of three experts from the RIVM and the National Institute of Mental Health and Addiction (Trimbos Institute), with considerable experience in various aspects (clinical, epidemiological, and managerial) of human viral hepatitis research. The project teams consist of doctors and researchers in close collaboration with the HepNed group, who coordinate the day-to-day activities and execute the actual retrieval. The pilot REACH project has provided significant knowledge with respect to planning, flow of communication, and development of technical, managerial, and production procedures that will be used to execute and improve CELINE.
Deliverables
There are 4 measurable deliverables for CELINE:
Identification of cases & establishment of the cohort
CELINE aims to establish a cohort of chronic HCV-infected patients who fulfil the following criteria: 1) diagnosed with chronic HCV after the year 2000, 2) persistent viraemia at time of CELINE assessment, 3) lost to follow-up from regular clinical care, and 4) residence in the Netherlands. The investigator-initiated pilot studies (preliminary data) cover the geographical healthcare areas of 10 hepatitis centres. The focus of CELINE will be the 37 remaining hepatitis centres in the Netherlands.
Based on the results from various Dutch pilot projects, the Centre for Infectious Disease Control (CIb, Het Centrum Infectieziektebestrijding) has issued a guidance directed to GGD on the most effective strategy to retrieve and re-evaluate chronic hepatitis patients. This lends governmental support to retrieval as a tool to reduce the burden of chronic HCV. The input of patients with every retrieval effort comes from various sources such as social and traditional media campaigns, general practitioners, laboratories, and the GGD.
Based on best practices, the most effective way to detect lost-to-follow-up patients is through reassessment of prior laboratory tests (positive anti-HCV and/or HCV RNA results) in all local and regional laboratories that perform virological testing for the hepatitis centre of interest. The virology laboratories in the Netherlands have filed their results digitally, which allow tracing of individual HCV test results performed up to 15 years ago. They are legally and ethically allowed to share data from all HCV-positive tested patients with clinicians, since they are seen as members of the treatment team.34 The treatment team has the obligation to provide the best patient care possible and retrieval is seen as an integral part of this responsibility. Clinical chart reviews are performed to ascertain follow-up and retrieve patient and disease characteristics necessary for the cohort registry. Most hospitals in the Netherlands currently have an integrated electronic patient management system, which enable physicians to follow the patient easily through the healthcare system. Current address information is requested from the Municipal Records Database, if possible. All retrieved patients are clinically assessed in one of the participating hepatitis centres, according to previously established screening protocols including a detailed interview; blood tests, including virology and genotyping; and transient elastography (Fibroscan) to evaluate liver fibrosis stage. After the screening visit, patients receive their test results together with a patient-tailored management advice. The results and outcome of patient counselling are shared with the general practitioner and further management and/or treatment according to current guidelines (the Dutch32 and/or EASL guidelines33) is planned. The choice of treatment regimen is dictated by the treating physician and will not be influenced by the researchers.
Registry
As part of CELINE, we built a dataset that includes data elements on routine demographics, such as route of transmission, co-morbidity, baseline viral load, HCV genotype, liver fibrosis assessments, prior treatment response (naïve, relapse, partial response, and non-response), virologic response to therapy, and therapeutic regimen. This is done as part of the HepNed nationwide registry for hepatitis C and is conducted in close collaboration with the Dutch HIV Monitoring foundation (SHM, Stichting HIV Monitoring).35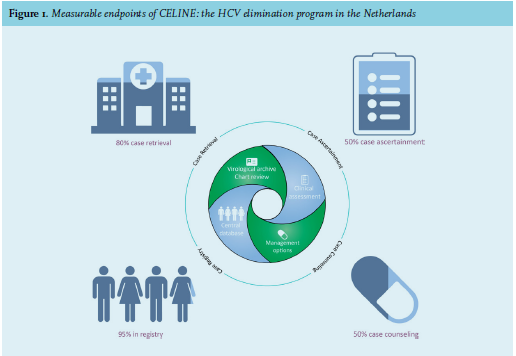
Expected outcome
In view of the pilot studies and the estimated size of the HCV population in the Netherlands, we estimate that CELINE will retrieve 4,000 patients and that ultimately 1,000 patients will commence DAA-based therapy (figure 1). CELINE has set a number of ambitious goals and indicates that in > 80% of 37 hepatitis centres, case retrieval will be completed as outlined in the working plan, and that in > 80% of the centres where the retrieval stage is completed, case ascertainment will be performed for > 50% of patients for whom a positive HCV laboratory test has been identified. Finally, the data of > 95% of patients who have been retrieved successfully will be entered into a central registry and > 50% of the patients who have had a complete case ascertainment will be provided case counselling.
CONCLUSION
The Netherlands is one of the countries with the lowest prevalence of chronic hepatitis C in Europe. There is a standard of healthcare, availability of DAAs, and the societal recognition to eliminate HCV; CELINE is well-positioned to perpetuate this momentum. Within the definitions set by the WHO, CELINE aims are to limit HCV complications, prevent new infections, and ultimately eliminate the disease. Modelling studies suggest that the Netherlands is an ideal battleground, giving us the opportunity to meet the WHO goals of 65% reduction in HCV-related mortality well before 2030. In doing do, we hope to become an example for other countries trying to reach this WHO goal. Achievement of HCV elimination (the ultimate WHO target) in Europe will require aligned regional and/or national strategies.
ACKNOWLEDGEMENTS
Funding: CELINE is supported through the HCV SCALE program: Screening Access and Linkage to CarE from Gilead Sciences.
Conflics of interest: MvD, PK and DP have no conflicts of interest. JA participated in advisory boards of Gilead, Janssen-Cilag, Bristol-Meyers Squibb (BMS), Abbvie, Merck Sharpe & Dohme (MSD), and ViiV and received research grants from BMS, Abbvie, and ViiV (all fees paid to institution). HB has participated in advisory boards of Gilead. DM has received honoraria for consulting/speaking from MSD, participated in advisory boards of MSD and received research grants from Gilead, Janssen-Cilag, BMS, MSD, and Roche. KE participated in advisory boards of Gilead, Janssen-Cilag, BMS, Abbvie, and MSD and received research grants from Gilead and Janssen-Cilag. BvH participated in advisory boards of Janssen-Cilag, BMS, Abbvie, MSD, and Norgine and received a research grant from Zambon Pharma. RdK has received honoraria for consulting/speaking from Gilead, Janssen-Cilag, BMS, Abbvie, MSD, Roche, and Norgine and received research grants from Gilead, Janssen-Cilag, BMS, and Roche. DR participated in advisory boards of BMS and Abbvie and received research grants from Abbvie. BR participated in advisory boards of Gilead, Abbvie, and MSD and received research grants from Gilead and MSD. JS participated in advisory boards of Gilead and received research grants from Gilead and Abbvie. SW has received honoraria for consulting/speaking from Gilead, Janssen-Cilag, BMS, and Roche, participated in advisory boards of Gilead, BMS, and Abbvie and received research grants from Gilead, Janssen-Cilag BMS, Abbvie, MSD, and Roche. MvdV has participated in advisory boards (fees paid to institution) of Abbvie, Gilead, Johnson & Johnson, MSD, and ViiV and has received independent research grants from Abbvie, Johnson& Johnson, Gilead, and MSD. JD declares that the Radboudumc, on behalf of JD, received honoraria or research grants from Novartis, Ipsen, Otsuka, Abbvie, and Gilead. JD served as consultant for Gilead and Abbvie, and in the last two years has been member of advisory boards of Otsuka, Norgine Gilead, BMS, Janssen, and Abbvie.
REFERENCES