KEYWORDS 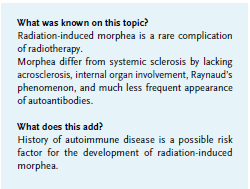
Radiation-induced morphea, Hashimoto’s thyroiditis, vitiligo, radiotherapy complications, multiple autoimmune diseases, localized scleroderma
INTRODUCTION
Radiation-induced morphea (RIM) is a rare cutaneous complication of radiotherapy. Little is known about the predictive risk factors for the development of this condition. In an attempt to highlight the role of autoimmunity in the pathogenesis of the disease, we present a woman with Hashimoto’s thyroiditis and vitiligo, who developed a radiation-induced morphea after radiotherapy for breast carcinoma.
To our knowledge, our case is the fourth report describing the association of morphea, Hashimoto’s thyroiditis and vitiligo,1-3 and the only one concerning the radiationinduced form of the condition.
OBSERVATION 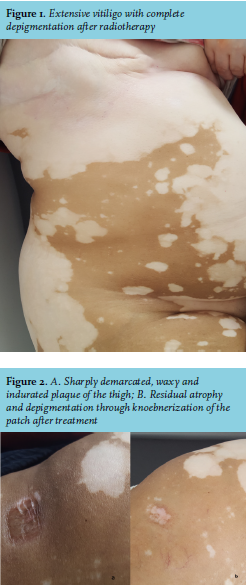
A 60-year-old woman was diagnosed with breast carcinoma in 2012. She had a right breast mastectomy and an axillary node sampling. She received three cycles of adjuvant 5-Fluorouracil (500 mg/m2) and cyclophosphamide (500 mg/m2), followed by three cycles of docetaxel (100 mg/m2). Adjuvant chemotherapy was followed by radiation therapy to her chest wall for a total dose of 50 Gy, 2 Gy per fraction, at a rhythm of one fraction per day, five days per week. She was placed on tamoxifen. Additionally, she was examined for a Hashimoto’s thyroiditis and increased values of thyroid peroxidase antibodies were detected. Finally, she presented with extensive vitiligo that began at least 10 years ago, and was aggravated by radiotherapy, as described below (figure 1). Four years ago, after radiotherapy was completed, the patient developed four asymptomatic sclerotic and atrophic well-circumscribed patches surrounded by lilac rings: one beyond the right inframammary area, in the right hypochondriac region; and three others on the left inframammary area, the abdomen and the thigh. Subsequent cutaneous biopsies demonstrated thickening and hyalinization of connective tissue of deep dermis, with perivascular and focal interstitial lymphocytic and plasma cell infiltrate. Laboratory investigations showed slightly positive antinuclear antibody test (1:80, speckled), but anti- SS-A/B, anti-Sm, anti-DNA and anti Scl 70 antibodies were all negative. Based on history, clinical presentation, laboratory and histopathological findings, we made a diagnosis of radiation-induced morphea.
The patient was treated with ultrapotent topical corticosteroids, resulting in the complete abolishment of lesions in the inframammary regions and abdomen, although residual atrophy and depigmentation through koebnerization remained in the patch of the thigh (figure 2).
DISCUSSION
Morphea, also known as localized scleroderma, is a rare inflammatory skin disorder that affects the skin and sometimes underlying subcutaneous tissue, muscles or bones. Morphea is clinically different from systemic sclerosis in that it lacks acrosclerosis, internal organ involvement and Raynaud’s phenomenon. Furthermore, antinuclear antibodies are detected in more than 85% to 95% of patients with systemic sclerosis, but are not a prominent feature of morphea.4
Morphea has been recognized as a complication of radiotherapy since the 1990s, mostly for breast cancer patients.5 Like the patient described above, it can develop several years after radiation therapy. To our knowledge, the disease has never been associated with autoimmunity. It is still unclear why RIM develops in some individuals. The strongest hypothesis proposes that antigens from altered endothelial cells, fibroblasts and collagen induce an immune response. This results in cytokine and growth factor production that stimulates the excessive creation of collagen.6 This reaction seems to be enhanced by the history of autoimmunity in our patient.
The extended delay in disease onset may be due to a cross-reactive immune response against radiation-induced antigens and some subsequent infections that occur several years later.
In this observation, radiation-induced morphea arose in a middle-aged woman, similar to most autoimmune diseases, in which a clear sex difference is observed. In addition, our patient’s condition was preceded by vitiligo and Hashimoto’s thyroiditis for several years, and the role of autoimmunity is well documented for these associated diseases.
Although not yet fully elucidated, autoimmunity is increasingly perceived as the underlying cause in the development of “spontaneous morphea”. This relationship is justified by three points: the association of some cases of morphea with an increased level of antinuclear antibodies;7 the familiar clustering of morphea and the coexistence of the morphea with multiple autoimmune syndromes.8-11 Morphea has been reported in association with Hashimoto’s thyroiditis and vitiligo in three cases.1-3 This particular case shows that radiation-induced morphea, like spontaneous morphea, can be associated to Hashimoto’s thyroiditis and vitiligo.
Treatment may prevent further progression of the disease but is not fully effective in reversing all disease damage; therefore, patients at risk of developing the morphea must be monitored, and early intervention is needed to prevent scaring.
CONCLUSION
No risk factors for the development of RIM are known to date, but we believe that a patient with a previous autoimmune disease treated with radiotherapy is at high risk for developing morphea. Hence, physicians should take extra precautions and treat the disease early to prevent unnecessary scaring.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES