D I A G N O S I S
First, the possibility of renal tuberculosis was considered. However, the patient had been treated adequately before transplantation and both the Ziehl-Neelsen and auramine staining for acid-fast bacteria were negative. Other causes of granulomatous tubulo-interstitial nephritis (GTIN) that were considered included acute T-cell mediated rejection, drug-related toxicity, infections, sarcoidosis, tubulointerstitial nephritis and uveitis syndrome, paraproteinaemia and Wegener’s granulomatosis. Finally, GTIN can be idiopathic.1
To find out if the histiocytic infiltrate in the biopsy was patient- or donor-derived, we performed fluorescent in situ hybridisation with probes directed to centromeres of the Xand Y-chromosome (the transplantation was from a male donor to a female recipient). This experiment showed that in the inflammatory infiltrate, both XX and XY cells were present. A double staining with CD68 indicated that the histiocytic cells were indeed donor-derived (figure 2). The diagnosis of donor-derived renal sarcoidosis was made.
The contralateral kidney of this same donor was also transplanted in another centre. In the pre-implantation biopsy a patchy infiltrate in the interstitium with giant cells and formation of granulomas without necrosis was present too.
Sarcoidosis is a chronic, idiopathic multisystem, inflammatory disease characterised by the presence of non-caseating granulomas in one or more organs, most often involving the lungs and hilar lymph nodes.1,2 Renal manifestations of sarcoidosis most commonly include hypercalciuria, nephrocalcinosis and nephrolithiasis as a result of a derangement in calcium homeostasis.1-3 Sarcoidosis may also directly involve the kidney in the form of GTIN. GTIN is unusual with a reported incidence ranging between 0.7 and 30%.3
Only ten cases of recurrent renal sarcoidosis in the form of GTIN in a renal allograft have been described previously.3 To the best of our knowledge, donor-derived, sarcoid granulomas in a renal allograft have never been described before.
Following the biopsy, her renal function recovered without additional treatment and she could be discharged from hospital in a good clinical condition two weeks after transplantation.
In conclusion, if GTIN is present in a recently transplanted kidney, clinicians should consider the possibility of donor-derived sarcoid granulomas and should not immediately attribute this finding to an acute T-cell mediated rejection. 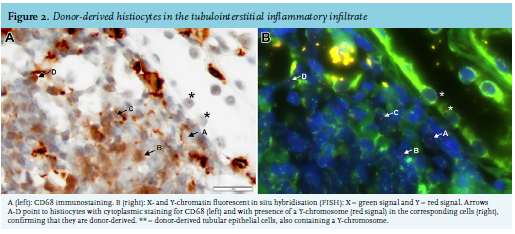
REFERENCES