CASE REPORT
A 79-year-old female of North African descent with end-stage renal disease caused by focal segmental glomerulosclerosis secondary to hypertension started intermittent haemodialysis in 2013. In 2014, she developed erythema nodosum, possibly due to latent tuberculosis infection (she tested positive for Mantoux and Quantiferon). Tuberculostatic treatment (rifampicin/ isoniazid) was started but then discontinued because of side effects (increasing malaise and gastrointestinal complaints). As latent tuberculosis infection is a relative contraindication for renal transplantation and the erythema nodosum relapsed, another attempt was made to treat her in 2016. She was successfully treated with isoniazid monotherapy for a duration of nine months.
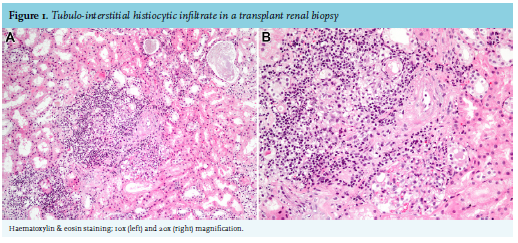
In April 2017 she received a first, deceased-aftercirculatory death donor kidney transplant from a 66-year-old male. The transplantation was complicated by delayed graft function. On postoperative day 6, a kidney transplant biopsy was performed. Light microscopy demonstrated tubulitis, possible arteritis, as well as acute tubular necrosis and mild mesangiolysis. Of note, in the tubulo-interstitial compartment, a patchy infiltrate consisting of lymphocytes and histiocytes was seen, with non-caseating granuloma formation (figure 1). Immunohistochemical staining for C4d was negative. The delayed graft function was attributed to the combination of acute tubular necrosis and tacrolimus nephrotoxicity. The tacrolimus dose was reduced.
WHAT IS YOUR DIAGNOSIS?
See page 386 for the answer to this photo quiz.