KEYWORDS
Antipsychotic agents, deep venous thrombosis (DVT), olanzapine, pulmonary embolism (PE), risk factors
INTRODUCTION
Olanzapine is a second generation antipsychotic (SGA) commonly prescribed for treatment of positive symptoms of schizophrenic patients. Common side effects of SGAs include diabetes, metabolic syndrome, sexual dysfunction, hyperprolactinemia and weight gain, the latter more frequently seen in olanzapine.1 A less known adverse event is that the use of olanzapine and other SGAs increase the risk of venous thromboembolism (VTE).1,2
VTE is a multifactorial disease with broadly two presenting entities: deep venous thrombosis (DVT) or pulmonary embolism (PE). Risk factors of VTE include immobility, sedation, previous VTE, active disease (e.g. infection or cancer), smoking, trauma, advanced age, male gender, hyperprolactinemia, antiphospholipid antibodies, obesity and certain genetic traits such as the factor V Leiden mutation.2
Both the Dutch website for drug information ‘Farmacotherapeutisch Kompas’ and the Dutch Summary of Product Characteristics (SmPC) of olanzapine mention VTE as an uncommon (0.1-1%) adverse drug reaction.3,4 The SmPC of olanzapine describes no causal relationship has been established and that patients with schizophrenia often have acquired risk factors for VTE. They recommend identifying all possible risk factors for VTE and taking preventative measures. The annual incidence of VTE is 1 per 1000 in adult populations.5 The risk of developing VTE is increased by 2.20 (odds ratio (OR), 1.22-3.95 (95% confidence interval (Cl))) in patients using SGAs.6
We describe a case of a young man with a history of paranoid schizophrenia who presented with a DVT in our hospital (the Maasstad Hospital in Rotterdam, the Netherlands) while using olanzapine. By appraising the reported cases in the databases of the Netherlands Pharmacovigilance Centre Lareb and VigiBase (the worldwide pharmacovigilance database maintained by the WHO collaborating centre for international drug monitoring UMC (Uppsala Monitoring Centre in Sweden)), we further explored the possible association between olanzapine and VTE. Lastly we performed a brief literature review on the potential mechanisms behind this association.
CASE REPORT
A thirty-year-old man was diagnosed with a DVT in our hospital in March 2016, six months after initiating olanzapine treatment. He was admitted to a long-term psychiatric ward for treatment of his therapy resistant paranoid schizophrenia and comorbid cocaine and amphetamines addiction.
In July 2015, he suffered from continuous hallucinations and delusions despite having been treated with several antipsychotics. The Dutch multidisciplinary guideline for Schizophrenia advises clozapine treatment when two different types of antipsychotics are not effective.7 However, our patient preferred olanzapine treatment and in August 2015 he was started on 300 mg olanzapine dosed by intramuscular injection once every four weeks.
By February 2016, he had gained 22 kg in weight (Body Mass Index (BMI) increase from 22.6 to 28.9) and had adopted a sedentary lifestyle, spending most of the day in bed. His high-density-lipoprotein (HDL) was reduced (0.83 mmol/l, reference level > 1 mmol/l) and his waist circumference had increased from 90 to 117 cm (reference < 102 cm). His blood pressure, glucose and triglyceride levels were normal. As only two out of five criteria obtained he did not qualify for metabolic syndrome.8
In March 2016, he presented at our hospital with a red swollen tender lower right leg. Ultrasound confirmed the diagnosis of DVT and the patient was started on anticoagulant treatment with a vitamin K antagonist with low molecular weight heparin injections until the desired prothrombin times were achieved. Risk factors for DVT in this patient were male gender, active psychosis, use of olanzapine, lethargy and high BMI after his significant and ongoing weight gain. Persisting psychotic symptoms and the presence of DVT made us decide to discontinue olanzapine and start clozapine. Within the next few months our patient became more active and less psychotic, however his BMI increased further to 31 kg/m2. Antithrombotic treatment was discontinued after three months, following the Dutch guidelines prevalent at that time.9
DISCUSSION
Other reports from Lareb and VigiBase
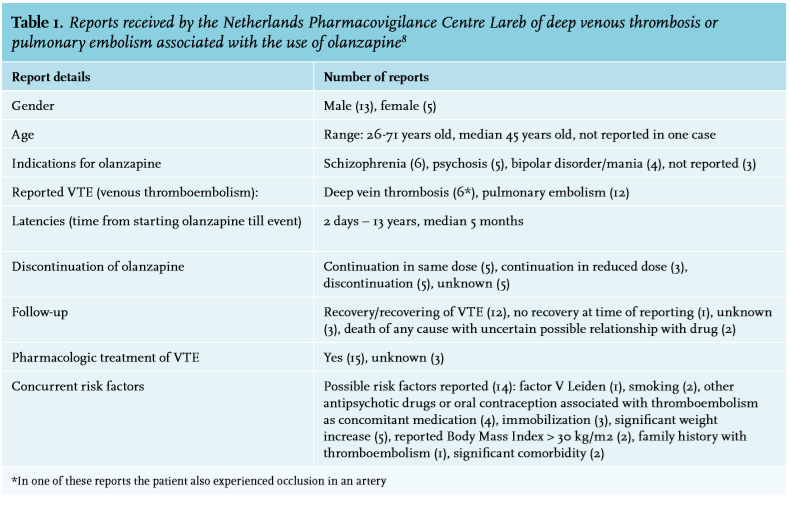
From 2001 to the 26th of January 2018 Lareb received 18 reports of DVT or PE associated with the use of olanzapine, including the previously discussed case report, see table 1 for further details.10 In 14 of these reports, patients had additional risk factors for VTE.
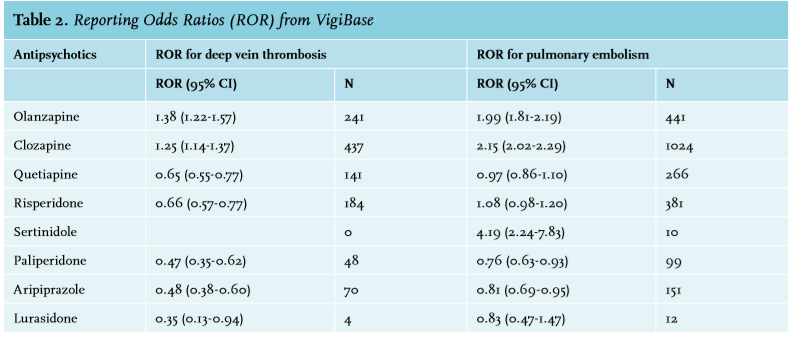
VigiBase lists 241 reports on olanzapine (with a Reporting Odds Ratio (ROR) of 1.38 [95% CI 1.22-1.57]) of the reaction ‘‘deep veinous thrombosis’’ (DVT) and 441 (ROR 1.99 [95% CI 1.81-2.19]) reports of the reaction ‘‘pulmonary embolism’’(PE), including the cases received by Lareb.11 The ROR is a measure of disproportional reporting in the database, and in this case a significantly increased ROR indicates that DVT or PE is more often reported for olanzapine use than with other drugs in the database. The ROR has been developed as a method for signal detection; it is therefore a hypothesis generating tool.12 The only other antipsychotic with a significantly increased ROR for these reactions was clozapine, with an ROR of 1.15 [95% CI 1.14-1.37, 473 reports] for DVT and an ROR of 2.15 [95% CI 2.02-2.29, 1024 reports) for PE. The RORs from VigiBase for various antipsychotics are described in detail in table 2.
Among the cases reported on in Lareb and VigiBase, the likelihood of a causal association between a drug and a reaction may vary as both are based on spontaneous reporting from various sources with different degrees of documentation.
Cases in the scientific literature
Various case reports in the scientific literature describe the association of olanzapine with VTE.13-16 Most case reports describe male patients aged sixty years and older, although PE has also been described in a 28-year-old male patient shortly after starting olanzapine treatment.16 Only a few population studies have reported on olanzapine specifically.6 A 2014 meta-analysis reports an OR of 1.35 (95% CI 0.97-1.89, p = 0.08) for the risk of VTE in patients using olanzapine. The results of this meta-analysis should be interpreted with caution since the quality and inclusion criteria varied between studies leading to between-study heterogeneity. This resulted in a low statistical power and a wide and nonsignificant confidence interval for all included SGAs.17 On the other hand a large case control study reported a significant OR for risk of VTE in patients using olanzapine of 1.49 (95% CI 1.07-2.08).18
Risk of VTE appears to be especially elevated in the first months of SGA treatment (OR 1.97; 95% CI 1.66-2.33). For users of antipsychotic drugs the risk was 56% higher compared to non-users (OR 1.56; 95% CI 1.39-1.75).19
However, current data can neither conclusively verify differences in occurrence rates of VTE between first- and second-generation antipsychotics nor identify which antipsychotic drugs have the lowest risk of VTE, though one might speculate that the risk of VTE is higher for clozapine than for other SGAs.20
Potential mechanism
The potential underlying mechanism explaining the higher risk of VTE during antipsychotic treatment is not yet fully clear. Various factors seem to play a role, especially metabolic syndrome, a common side effect of olanzapine treatment as 34% of schizophrenic patients taking olanzapine monotherapy fulfil its criteria.21 Metabolic syndrome is a known risk factor of VTE.22
Immobilisation, a consequence of the lethargy caused by various antipsychotics, is linked to increased risk of VTE due to venous stasis and blood pooling in the lower extremities. Obesity is also an independent risk factor for VTE and although all SGAs are associated with some weight gain and increased appetite, olanzapine and clozapine have the most profound impact compared to non-SGA antipsychotics and placebo.23-25 A database analysis comprising 3507 patients in 21 placebo- and active-controlled studies conducted in America, Australia, New Zealand and Europe showed that 48% of patients taking olanzapine experience > 7% weight gain within the first 12 weeks, and 57% of patients experience a significant weight gain within the first 6-12 months with a median weight gain of 0.7 kg per month, compared to placebo (incidence of weight gain in placebo was 13%).24 This increase in body weight of at least 20% is more pronounced in inexperienced users of antipsychotics.25 Only in olanzapine users a significant increase in weight was found when comparing the weight at > 38 weeks to the weight at six weeks after starting olanzapine.25 Therefore, if a patient is already on olanzapine, switching to a different antipsychotic drug, such as haloperidol, might be indicated.26 In one case, switching from olanzapine to asenapine resulted in 6.6% weight loss without further impairment of psychological functioning.27
There is less information available regarding the presence of lethargy in schizophrenic patients treated with antipsychotics. It is difficult to compare trials as they do not always give a clear description of somnolence, sedation, lethargy and hypersomnia. Nevertheless olanzapine, quetiapine, risperidone and especially clozapine are all associated with significantly more of these symptoms compared to placebo.28 About 25-39% of patients taking olanzapine experience sleepiness, which is significantly more than placebo (26.2% compared to 15.3%), whereas somnolence is experienced by 26-46% of patients taking clozapine.28,29 It has been postulated that in antipsychoticinduced somnolence blockade of histamine 1 receptors and α1 receptors play an important role.30,31
Other associated risk factors include raised levels of antiphospholipid antibodies and hyperprolactinemia. The exact roles of these risk factors in a clinical psychiatric setting still need to be determined.32
It is Hypothesiezed that antipsychotics directly influence the risk of VTE, in particular second generation antipsychotics such as clozapine and olanzapine. Many antipsychotics antagonise the serotonin (5-HT2A) receptors. As these receptors are also present on platelets, the antipsychotic medication might influence platelet aggregation.33 Paradoxically, most studies investigating this mechanism suggested a lower risk of VTE.
Almuqdadi et al. have shown that risperidone, and not olanzapine, leads to a clinically significant inhibition of platelet aggregation induced by serotonin. When adding these antipsychotics to a serotonin-epinephrine combination, both weak platelet agonists affecting respectively the 5-HT and the α2A-adenergic receptors on platelets, a dose-dependent inhibition of platelet aggregation was found. However, no statistically significant inhibitory effect on platelet aggregation was seen with olanzapine, possibly due to a lower 5-HT2A and α2A-adenergic receptor affinity compared to e.g. risperidone.31 Another in vitro study indicates that clozapine and olanzapine show a strong inhibitory effect on ADP-stimulated platelet aggregation, which would also lower the risk of VTE.34 Yet another in vitro study has shown increased platelet adhesion and aggregation for clozapine, but not for olanzapine.32
These results suggest that the serotonin receptor effect does not account for the increased risk of VTE while using SGA. In absence of a clear pathogenic mechanism to account for the associated higher risk of VTE in olanzapine users, we might conclude that this association is most probably caused by risk factors like substantial weight gain and lethargy, not by olanzapine itself.
Diagnosing VTE in psychiatric patients
VTE is known to have a diagnostic delay, the average delay in diagnosing PE is 8.6 days, where patient delay is on average 4.2 days and delay in primary care is 3.9 days on average.35 23.8% of patients are diagnosed at least a week after onset of symptoms. The absence of chest symptoms is associated with a diagnostic delay with an OR of 5.4 (95% CI 1.9-15).36 Specifically, patients with a diagnostic delay were less likely to present with chest pain (24% vs 54%, p = 0.003) or pain during inspiration (9% vs 33%, p = 0.011) compared to patients without diagnostic delay. Pain perception in schizophrenic patients is impaired in various ways, without an exact mechanism being clear.37 Also, cognitive impairment and excess negative symptoms influence the expression of pain in this patient category.38 For example, in a case report of a 75-year-old patient diagnosed with catatonic schizophrenia and with PE the patient could not express any pain symptoms, which stresses the fact that schizophrenic patients are more likely to have diagnostic delay in the diagnosis of VTE.39 As venous thromboembolism is an important cause of mortality and morbidity is it important to take this into account. An observational study including systematic venous ultrasound identified DVT in 10 out of 449 patients (2.2%) after 10 days admission to a psychiatric ward. Within 90 days 17 patients developed VTE including three symptomatic PEs.40
Options for prophylactic treatment
Identifying patients on antipsychotic therapy who have a high risk of developing a VTE might be difficult as no validated risk score is available that is able to detect which psychiatric patients might benefit from pharmacologic VTE prophylaxis. For olanzapine use alone, an OR of 1.35 for the risk of venous thrombosis does not seem to justify prophylactic treatment with low molecular weight heparins (LMWH). However, additional risk factors for VTE have been identified in psychiatric patients.
One risk score designed specifically for psychiatric patients includes the use of antipsychotics.41 Other risk factors included are history of VTE, cancer (active/treated), age, acute infectious/respiratory disease, immobilization (including catatonia), hormone therapy, obesity (BMI > 30), dehydration and thrombophilia. Based on the presence of these risk factors patients could be categorized according to their low, medium or high risk of developing a DVT with the recommendation to start LMWH in the medium and high risk populations. However, this risk score and the algorithm derived from it have not yet been validated in a larger setting and it is unclear whether the benefits of the prophylactic treatment with anticoagulants (e.g. LMWH) outweigh possible side effects, for example an increased risk of bleeding.
The Padua risk score has been validated in a larger clinical setting of medical inpatients and has been proven to distinguish between inpatients with high risk of VTE and patients with low risk. The risk factors involved are active malignancy, previous VTE, immobility, thrombophilia, trauma and/or surgery less than one month ago, age over 70 years, cardiovascular and or respiratory diseases, acute infection and or rheumatologic abnormalities, a BMI of more than 30 and hormonal therapy.42 Nevertheless, this model was not specifically tested in psychiatric patients and only in an acute hospital setting.42 Therefore we also cannot use the Padua risk score in a psychiatric ward for deciding on whether to give pharmacological prophylactic treatment.
CONCLUSION
SGAs such as olanzapine are commonly prescribed for treatment of positive symptoms of schizophrenia, but are associated with a higher risk of VTE. This association is most likely explained by associated risk factors such as substantial weight gain and lethargy, both side effects of olanzapine. Further studies are required to determine the potential mechanisms of olanzapine on for example thrombogenicity and platelet aggregation.
In general, it is important to realise that diagnosing VTE in schizophrenic patients can be more difficult, due to symptoms such as lethargy and impaired pain perception. No validated risk score is available for detection of psychiatric patients who might benefit from pharmacological VTE prophylaxis. In patients who develop VTE while being treated with a SGA such as olanzapine, discontinuation of olanzapine might be considered based on individual risk profile, control of psychotic symptoms and antipsychotic treatment options.
DISCLAIMER
The authors are indebted to the national pharmacovigilance centres that contributed data to VigiBase, maintained by the World Health Organization (WHO) collaborating centre for international drug monitoring UMC (Uppsala Monitoring Centre in Sweden). The opinions and conclusions, however, are not those of the various centres, nor of the UMC in Sweden. The information originates from a variety of sources, and the likelihood that the suspected AEs are drug-related may vary between cases.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES