DIAGNOSIS
Radiotherapy-induced arterial occlusion of the superior mesenteric artery (SMA) and the celiac trunk.
The absence of abnormalities of the vessel walls in other arteries, the specific location of occlusion in the radiated tissue and the age of the patient suggested that the arterial occlusion was a late complication of radiotherapy which he underwent ten years earlier. The history of nicotine and drug abuse and psychiatric comorbidity suggested that in the early stage, the abdominal pain was caused by a psychiatric disturbance, and this delayed the further diagnostic process. Smoking and intravenous drug abuse may have accelerated the process, but are unlikely to be the sole cause of localised abdominal arterial occlusion. The intervention-radiologist performed a difficult percutaneous transluminal angioplasty with stent placement (Express SD 6x19mm, Boston Scientific) in the SMA the next day (figure 2) through brachial access. During this long procedure the patient was conscious and because of agitation we decided stop after stenting the SMA.
Radiotherapy-induced arterial damage was first described in 1899.1 Studies show that arterial occlusion is rare and can develop many years after radiotherapy, intervals ranging from 4 to 44 years after treatment.2 It is notable that advanced local occlusion can be present without any signs of arterial damage in other large arteries. Arterial occlusion in the irradiated area, with sparing of the non-radiated areas, is highly suggestive of radiotherapy-induced arterial occlusion. The pathogenesis of radiotherapy-induced arterial stenosis is similar to that of accelerated atherosclerosis and can be seen in young patients many years after radiotherapy.3
Early revascularisation is important to prevent bowel ischaemia. Most patients with coronary or femoral occlusion after radiotherapy show slowly progressive nonspecific symptoms.5 When found early, revascularisation is successful in most cases.5 Intervention can be difficult, due to fibrotic changes and a slow recovery of the vessel wall in the radiated area. Surgical intervention of arterial occlusion is often complicated due to early re-occlusion. Stenting of the artery can be challenging, but seems the appropriate and preferable treatment of radiation-induced arterial occlusion.6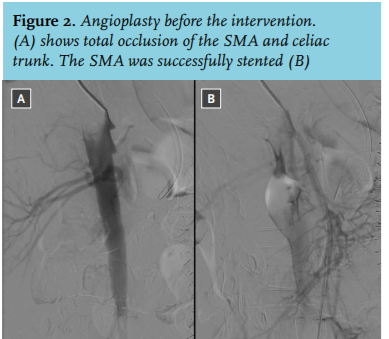
CONCLUSION
Although arterial occlusion is rarely seen as a result of radiotherapy, it can be a serious and potentially lethal complication. It needs to be stressed that although other diseases may be distracting, it is important to be certain of the full medical history of the patient to prevent early mortality in young patients who have undergone radiotherapy.
DISCLOSURES
All authors declare no conflict of interest.
REFERENCES