KEYWORDS
Asthma, high-altitude climate therapy, predictors
INTRODUCTION
Severe asthma is a life-threatening disease currently understood to be a complex interaction of clinical, physiological and inflammatory characteristics resulting in different phenotypes. Over the last decade studies have identified at least three different phenotypes for severe asthma, including severe atopic asthma, persistent eosinophilic asthma (formerly called ‘intrinsic’ asthma) and asthma associated with morbid obesity.1-4 This phenotypic heterogeneity is mirrored by different responses to asthma treatment. For example, persistent eosinophilic asthma usually responds to high-dose inhaled or oral corticosteroid treatment,1 whereas the obese phenotype typically does not,5 which supports the need for targeted treatment.6,7
Apart from new biological pharmacological targeted treatments,8,9 also non-pharmacological treatment strategies such as directly targeting airway smooth muscle with bronchial thermoplasty,10 optimising the management process with telemonitoring,11 or treating the patient in a low-trigger environment at high altitude12 have been shown to be beneficial for patients with severe asthma.
High-altitude climate therapy involves exposure to conditions of altitude ≥ 1500 metres above sea level.13 It was previously believed to be of benefit specifically for patients with atopic asthma14 but recent evidence shows that atopy is not the only driver for a successful outcome.15-18 The determinants of a successful outcome of high-altitude climate therapy are still unclear. From clinical experience it appears that also the type of response to high-altitude climate therapy differs between patients. Some have a more pronounced improvement in lung function,13 whereas others boost their exercise tolerance or are able to taper their dose of oral corticosteroids.
In the present study, we investigated whether typical clinical, functional and inflammatory characteristics of patients with severe asthma can predict a specific beneficial outcome of high-altitude climate therapy.
MATERIAL AND METHODS
Patients and design of the study
This is a secondary analysis of a prospective cohort study evaluating patients with severe, refractory asthma who were referred to the Dutch Asthma Centre in Davos, Switzerland, in order to optimise their disease. The Dutch Asthma Centre is localised at an altitude of 1600 meters above sea level and offers personalised, multidisciplinary, multifaceted treatment for patients with severe asthma in a low-trigger environment. The characteristics of the cohort have been described previously.12 In short, participants were adult patients (17-75 years) with a diagnosis of severe refractory asthma using high doses of inhaled corticosteroids ≥ 1000 µg/day of fluticasone or equivalent or chronic oral corticosteroids, combined with long-acting bronchodilators for at least one year. Current smokers and patients with a history of more than 15 pack-years of cigarette smoking were excluded from the study. All patients were symptomatic and had had at least one severe exacerbation during the past year requiring a course of oral corticosteroids.
The study was approved by the Ethics Committee of the Academic Medical Centre of the University of Amsterdam (Amsterdam, the Netherlands) and was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent before taking part in the study. This study was registered at the Netherlands Trial Register, www.trialregister.nl under NTR 1277.
Assessments
Patients participating in this study were assessed and evaluated according to a systematic protocol at entry and after 12 weeks of treatment.
Questionnaires
At baseline, all patients completed standard questionnaires including information on socio-demographics, asthma history, current symptoms, smoking habits and medication usage, including daily doses of inhaled and oral corticosteroids.
The level of asthma control was assessed using the Juniper ACQ-6 score, a 6-item version of the Asthma Control Questionnaire with the FEV1 question omitted.19 In this questionnaire, patients recall their experiences over the past seven days and respond to each question on a 7-point Likert scale, where 0 represents no impairment and 6 represents maximum impairment.
Asthma-related quality of life was measured using the Juniper Asthma Quality of Life Questionnaire (AQLQ), an asthma-specific questionnaire that measures symptoms, activity limitations, emotional functioning, and environmental stimuli.20 The mean of the 32 items in the AQLQ between 1 (very poor asthma-related quality of life) and 7 (best asthma-related quality of life) was used. The 20-question Sino-Nasal Outcome test (SNOT-20) was used to measure rhino-sinusitis-related quality of life. The mean total score ranges from 0 (no symptoms) to 5 (severe symptoms) and is calculated by averaging an individual’s responses to all questions.21
The severity of fatigue was measured by the subscale Subjective Fatigue from the multidimensional Checklist Individual Strength (CIS).22 The Subjective Fatigue subscale of the CIS (CIS-Fatigue) consists of eight items, scored on a 7-point Likert-scale, higher scores meaning worse outcomes.
Lung function assessment
Pulmonary function testing was performed using the Masterscreen PTF (Jaeger Viasys, Germany). Forced expiratory volume in one second (FEV1) was assessed before and after inhaled administration of 400 µg salbutamol and expressed as percentage of predicted value.23
Exercise tolerance
The six-minute walk test (6MWT) measures the maximum distance an individual is able to walk on a flat, hard surface in a period of 6 minutes.24 The self-paced 6MWT assesses the submaximal level of functional capacity of the patient and reflects the functional exercise level for daily physical activities. An improvement of 54 meters has been shown to be a clinically important difference.25
Assessment of allergy and inflammation
Total IgE and specific IgE to common aero-allergens (house dust mites, mixed grass and birch pollen, cat and dog dander and Aspergillus fumigatus) in peripheral blood was assessed by fluoro-enzyme immunoassay UniCAP® (Pharmacia & Upjohn, Uppsala, Sweden) and expressed in kU.L-1. Eosinophils in peripheral blood were measured by a standard automated cell counter. Fractional exhaled nitric oxide (FeNO) was measured by a chemiluminescence analyser (Niox Aerocrine AB, Solna, Sweden) according to the current guidelines.26
Potential predictors of benefit
Nineteen baseline demographic, clinical, functional, and inflammatory parameters were selected as the most clinically relevant and considered as potential predictors of favourable or unfavourable outcome.
Outcomes
Five outcomes considered to be representative of five clinically relevant domains of improvement were defined: change in oral corticosteroid dose (medication requirement domain), change in AQLQ score (patient-reported outcome domain), change in FEV1 (lung function domain), change in blood eosinophils (airway inflammation domain) and change in BMI (lifestyle domain). The choice of these outcomes was based on literature about clinical phenotypes of severe asthma in adults.1-4
Statistical analysis
Changes from baseline in BMI, daily oral corticosteroid dose, AQLQ score, FEV1, and peripheral blood eosinophils were analysed using paired t-test or Wilcoxon signed-rank tests, depending on the distribution of the variables.
Spearman rank-order correlation was used to explore the association between the potential predictors of benefit and each of the outcomes. Predictors with a statistical significance (p value < 0.05) were included in the multiple linear regression analysis to identify independent predictors of benefit. Analyses were conducted using PASW Statistics 20.0 (SPSS, Inc., Chicago, IL, USA). 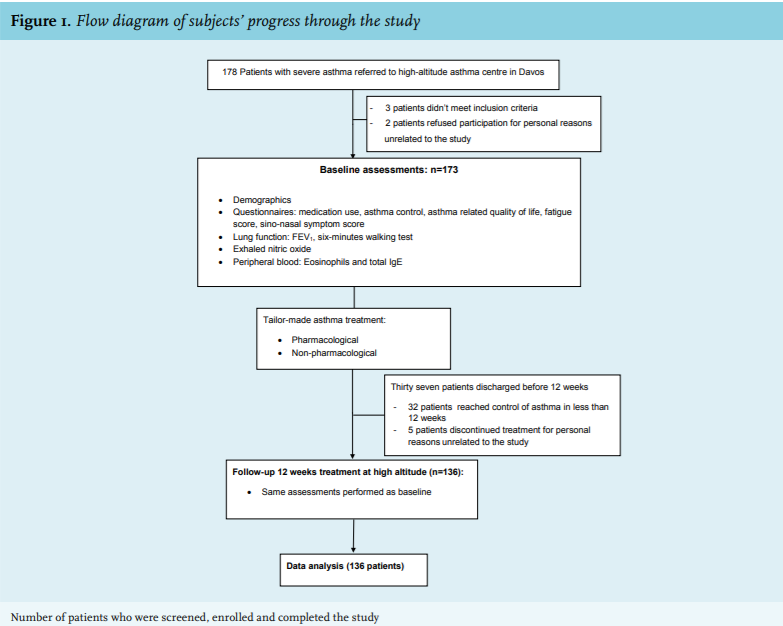
RESULTS
A total of 173 patients participated in the study. Of these, 136 patients had assessments performed at baseline and at 12 weeks of treatment, and were included in the analysis (figure 1). Thirty-seven patients were only assessed at baseline, but not at 12 weeks for variable reasons: 32 patients achieved control of asthma and were discharged home before 12 weeks and 5 had the high-altitude treatment discontinued for personal reasons.
There were no differences in baseline characteristics between patients who did and did not finish the study (data not shown).
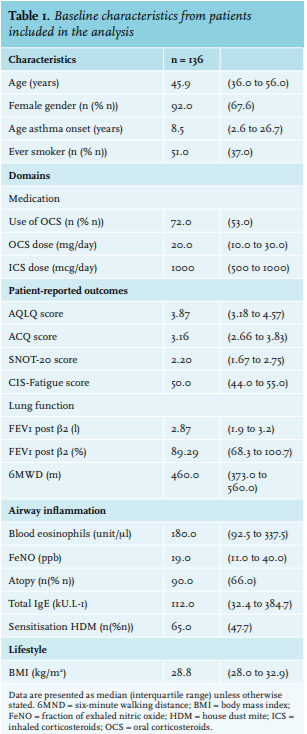
Baseline characteristics are shown in table 1. Changes from baseline in the five main outcomes are shown in table 2.
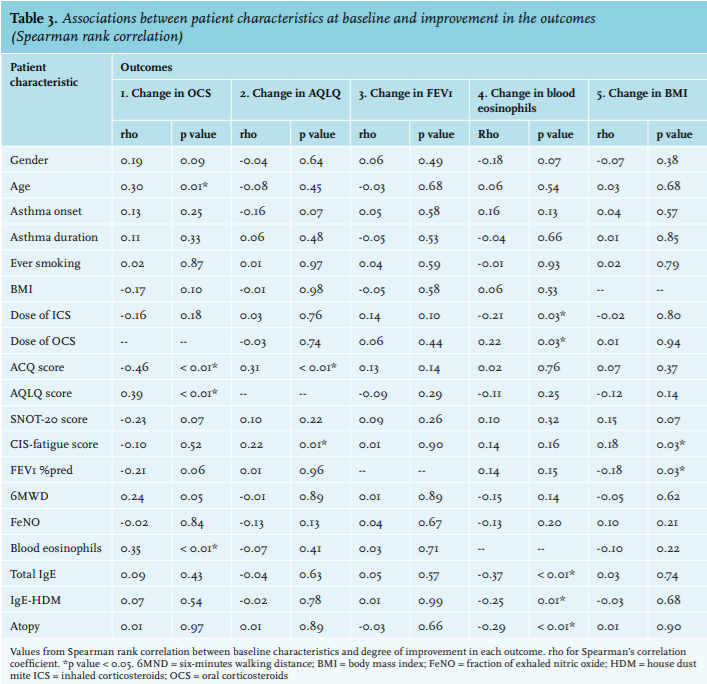
Predictors of benefit from high-altitude treatment
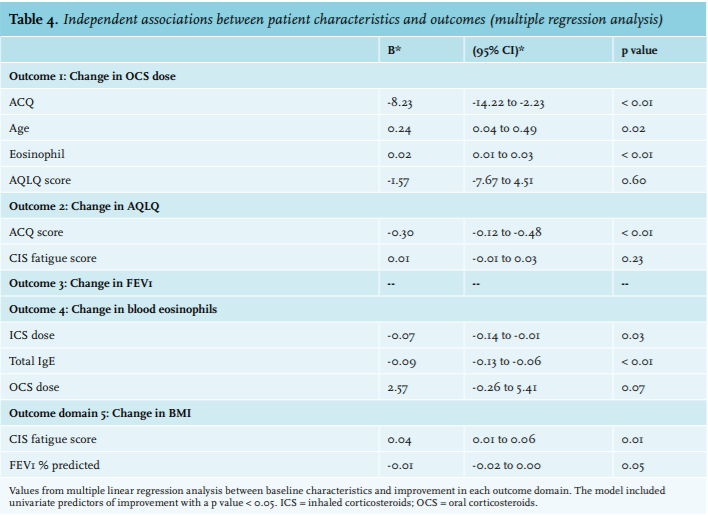
Spearman rank correlations between potential predictors of improvement (baseline characteristics) and each outcome are listed in table 3. All patients showed improvements in AQLQ and FEV1 at 12 weeks, but no specific predictors for improvement of these parameters were identified. Poorer asthma control (p < 0.01), younger age (p = 0.02) and lower blood eosinophil counts at baseline (p < 0.01) were independently associated with reduction in daily oral corticosteroid dose at 12 weeks. Higher inhaled corticosteroid dose (p = 0.03) and high total IgE at baseline (p < 0.01) were independently associated with reduction in blood eosinophils at 12 weeks and a lower fatigue score at baseline was independently associated with reduction in BMI (p = 0.01) (table 4). 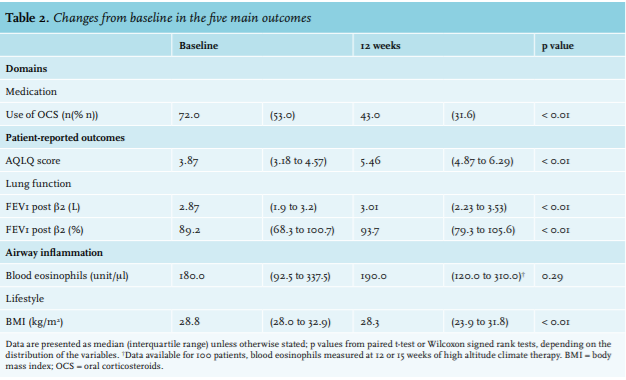
DISCUSSION
In this study we categorised the benefits of high-altitude climate therapy for patients with severe asthma in five different outcome domains represented as reduction in daily oral steroid use, improvements in asthma-related quality of life, FEV1, blood eosinophils and weight loss. Each of these outcomes was independently associated with specific patient characteristics, except for the improvement in asthma-related quality of life and FEV1, which was similar for all patients with severe asthma.
Nearly all patients with severe asthma participating in this study showed a significant improvement in their asthma-related quality of life scores after high-altitude climate therapy. No patient characteristics could predict this benefit, which suggests that non-specific aspects of high-altitude climate therapy played an important role, such as better air quality, improved adherence with the drug regimen or removal from stress at home or at the workplace.27 Therefore, high-altitude climate therapy might be an option for patients with severe refractory asthma, irrespective of their phenotype.
The majority of the prednisone-dependent patients were able to reduce their dose of oral corticosteroids after 12 weeks of high-altitude climate therapy while maintaining the same level of asthma control. The degree of oral corticosteroid reduction was associated with higher symptom score and younger age, combined with low blood eosinophil count at baseline. Similar characteristics were described by Haldar and colleagues in the highly symptomatic, low eosinophilic non-obese asthma phenotype.1 This suggests that these patients were symptomatic for other reasons than severe airway inflammation and reinforces previous studies which demonstrated that tapering of oral corticosteroids is easier in patients without eosinophilia.28
For the group as a whole there was a significant improvement in post-bronchodilator FEV1, up to 10% of the predicted value in some patients. A previous meta-analysis had also demonstrated benefit of high-altitude climate therapy in the lung function of adult patients with asthma.13 However, we could not find any clinical or inflammatory predictors of improvement. A reduced post bronchodilator FEV1 indicates persistent airflow limitation, probably linked to inflamed and swollen airway mucosa or airway remodelling. A possible explanation could be that high-altitude climate therapy reduces the thickness of the airway mucosa or might even reverse airway modelling, irrespective of the patient characteristics at admission, but this remains to be investigated in future studies.
Blood eosinophils did not change significantly for the group as a whole, which may be explained by a simultaneous tapering of anti-inflammatory medication. Still, there were patients showing significant reductions of blood eosinophil levels, suggesting an anti-inflammatory effect of high-altitude climate therapy in selected patients. Predictors of such a reduction in blood eosinophils were a high level of total IgE and a high level of inhaled and oral corticosteroid use. This fits with the hypothesis that continuous exposure to allergens (e.g. house dust mites, fungi) at sea level had been responsible for ongoing airway inflammation and elevated blood eosinophil counts despite high dose anti-inflammatory treatment.27 At high altitude these triggers were likely to be either absent or largely diminished. Thus, in patients with high IgE levels, even if already treated with high doses of anti-inflammatory medications, objective improvement in systemic inflammation can be obtained by high-altitude climate therapy.
In our study, more pronounced weight reduction was associated with lower fatigue scores at baseline, indicating that patients with more vitality had more possibilities to reduce weight by physical activity. Many studies have shown that weight reduction improves clinical outcomes in patients with asthma.29,30 but it is not always easy to achieve a significant weight reduction in patients with asthma and obesity with lifestyle modification and physical exercise at sea level. Our study suggests that physical activity might be facilitated in a clean air environment with multidisciplinary support and therefore might help patients with severe asthma to improve their physical condition and subsequently reduction of BMI.
This study has a few potential limitations to be addressed. Firstly, some patient characteristics that could also have influenced treatment outcomes have not been addressed, such as stressful psychosocial conditions, hormonal changes (adrenal gland activation)31 and unknown exposures to sensitising agents. In particular anxiety and depression might have been important predictors of beneficial response, since it has been shown that these are important contributors to asthma severity.32 If so, our data suggest that high-altitude climate therapy could have had a beneficial effect on these psychological stressors as well. Secondly, altitude itself could have influenced the partial pressure of gases such as FeNO with potential overestimation of FeNO levels.33 However, we believe that this did not influence our findings since change in FeNO was not used as an outcome, and baseline FeNO was included as a continuous variable in the regression analyses.
Thirdly, this study was a one-centre intervention and although previous studies on high-altitude climate therapy in children and adults showed similar improvements,15-17 extrapolation of our results to other high-altitude centres cannot be easily done.
Furthermore, although the current study was not designed to compare high-altitude climate therapy with similar in-house treatment at sea level, it would have been worth evaluating the effect of a similar program at sea level for these patients. A prospective comparative study is currently ongoing in the Netherlands (NTR5182).
Finally, some parameters (total IgE, blood eosinophils, 6-minute walking distance) were not assessed on two occasions in all patients, which might have affected the power of our study. Still, meaningful results could be obtained, despite this potential lack of power.
CONCLUSION
In conclusion, this study shows that high-altitude climate therapy improves quality of life and lung function in all patients with severe asthma. Maintenance oral steroid use, body weight, and blood eosinophils improve to a variable extent depending on patient characteristics, such as age, degree of asthma control, total IgE and fatigue score before admission. For clinicians these results show that the benefits of high altitude are multiple and diverse, and that for each patient with severe asthma a specific treatment target can be formulated. Identifying predictors of improvement of high climate therapy is the first step toward understanding mechanisms of the different phenotypes of severe asthma, as well as the beneficial effects of a low-trigger environment.
ACKNOWLEDGMENTS
The authors thank all study participants for their valuable contribution. The Netherland-Davos Society supported the Merem Dutch Asthma Centre Davos in the performance of this research. The funding sources had no role in the study design, data collection, analysis or interpretation, or in the decision to submit this article for publication.
DISCLOSURES
The authors report no conflict of interest relevant to the content of this report.
REFERENCES