KEYWORDS
Adverse drug reaction, direct oral anticoagulants, cholesterol crystal embolisms
INTRODUCTION
The direct oral anticoagulants (DOACs) dabigatran (Pradaxa®), rivaroxaban (Xarelto®), apixaban (Eliquis®) and edoxaban (Lixiana®) are indicated for the treatment of venous thromboembolisms and prophylaxis of venous and arterial thromboembolisms. Dabigatran directly inhibits thrombin. Apixaban, edoxaban and rivaroxaban inhibit the coagulation factor Xa. Dabigatran and rivaroxaban were granted marketing authorisation in the Netherlands in 2008, apixaban in 2011 and edoxaban in 2015.1-4
Cholesterol crystal embolisation (also referred to as cholesterol embolisation syndrome, atheromatous embolisation or atheroembolism), refers to cholesterol crystals originating from an atheromatous core of an atherosclerotic plaque in a large artery, embolising to a distant medium or small artery, leading to mechanical obstruction and inflammation resulting in end-organ damage. Usually several small emboli (microemboli) are released over time. The possible end-organ damage includes renal failure, skin manifestations such as the blue toe syndrome or small cerebral infarctions. The inflammatory response may lead to fever and hypereosinophilia. The diagnostic hallmark is a biopsy showing intravascular cholesterol crystals. Cholesterol crystal embolisation may occur spontaneously or after arterial or other surgical interventions. Thrombolytic and anticoagulant treatment are also associated with cholesterol crystal embolisation, but it is still uncertain whether these are independent risk factors.5,6
This article describes cases concerning DOACs associated with cholesterol crystal embolisms from the spontaneous reporting database in the Netherlands maintained by the Netherlands Pharmacovigilance Centre Lareb, the European Pharmacovigilance database EudraVigilance maintained by the European Medicines Agency (EMA), and one case published in the scientific literature. It must be noted that cases from pharmacovigilance databases concern spontaneous reports of possible adverse drug reactions reported by healthcare professionals, manufacturers, patients or others, and the likelihood of a causal relationship can differ between cases.
CASE SERIES
Details of the cases are described below. A summary of the cases is listed in table 1.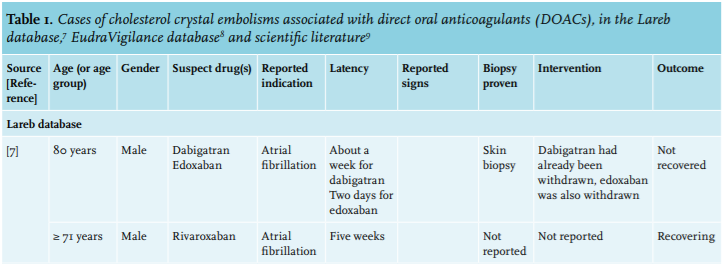

Cases received by Lareb
The Netherlands Pharmacovigilance Centre Lareb received two reports of cholesterol crystal embolism associated with the use of a DOAC.7
One case concerned an 80-year-old male. The medical history included aortic graft surgery, myocardial infarction treated with coronary angioplasty, multiple transient ischaemic attacks and atrophy of the left kidney. About one week after starting a DOAC (initially treatment with dabigatran and after five days replacement by edoxaban) for atrial fibrillation, the patient noticed blue discolouration of the toes. At physical examination blue toes and levido reticularis were seen, and the possible diagnosis of cholesterol crystal embolisms was suspected. Laboratory evaluation revealed leucocytes of 7.0 x 109/l with slightly elevated eosinophils of 0.7%. Blood creatinine had increased from 140 to 230 µmol/l, with a decrease of MDRD from 41 to 22 ml/min/1.73 m2. Urinary analysis showed no proteinuria and no urinary sediment abnormalities. At kidney ultrasound there were no visible changes compared with previous investigation. Skin biopsy was performed, and confirmed the diagnosis of cholesterol crystal emboli. Edoxaban was withdrawn. At the moment of reporting, the patient had not recovered. Concomitant medications were pantoprazole, ezetimibe, metoprolol, losartan and rosuvastatin.
The other case concerned a male in the age group 71 years and older, with cholesterol crystal embolisms following administration of rivaroxaban for atrial fibrillation with a latency of five weeks after start. The patient experienced a blue toe, which spontaneously recovered, while continuing the use of rivaroxaban. Concomitant medications were sitagliptin, glimepiride, amlodipine and atorvastatin.
EudraVigilance cases
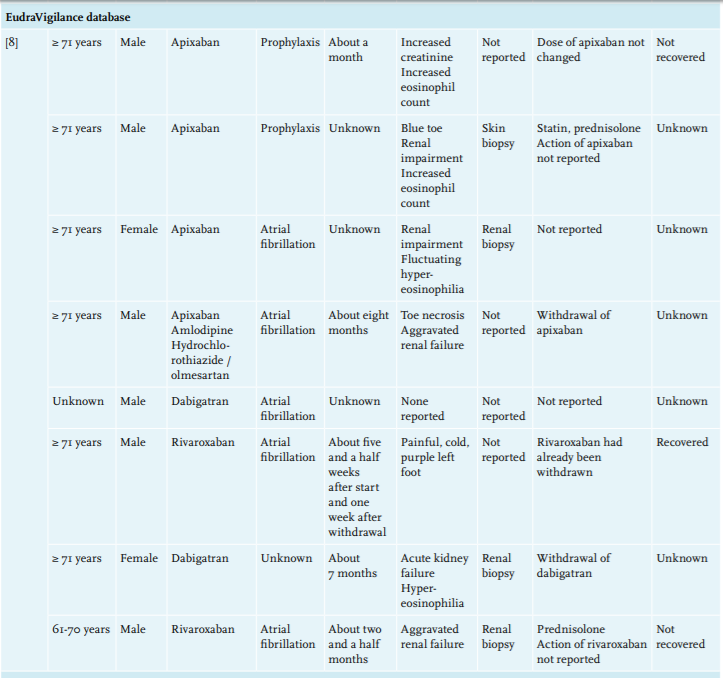
When excluding the Lareb cases, the European Pharmacovigilance database EudraVigilance contained another eight strongly supportive cases of a DOAC associated with cholesterol crystal embolisms.8 The reports concerned six men and two women. Ages varied from 70 up to and including 81 years (mean and median 78 years), where in one report only the age ‘in his 70s’ was reported and in one patient age was unknown. Suspect drugs were dabigatran in two reports, rivaroxaban in two reports and apixaban in four reports. In one report amlodipine and hydrochlorothiazide were also mentioned as suspect drugs. In the other seven reports the DOAC was the single suspect drug. Other possible causes of cholesterol crystal embolisms such as arterial or other surgical interventions were not described in the reports. Latencies were reported in five cases, varying from one month to eight months after start of the DOAC. One report described that cholesterol crystals were observed in a skin biopsy specimen, and three other reports in a kidney biopsy specimen. In three reports the presence of eosinophilia was mentioned.
Case in scientific literature
In the scientific literature one other case was described of cholesterol crystal embolisms associated with the use of a DOAC. This case concerned a 79-year-old male, whose medical history included hypertension and hyperlipidaemia, who developed acute renal failure six weeks after start of dabigatran for atrial fibrillation. Peripheral eosinophils were elevated. Renal biopsy showed cholesterol embolisms. Dabigatran was withdrawn. Renal function did not recover.9
DISCUSSION
Cholesterol crystal embolisms were described in association with the use of several other antithrombotic drugs including heparin, low-molecular-weight heparin, warfarin, and thrombolytic therapy.10-13 The cholesterol embolisation syndrome may occur four to eight weeks after anticoagulation therapy in patients with underlying atheromatous disease.14
The role of anticoagulants as an independent risk factor for cholesterol crystal embolisms is, however, not conclusive.15-17 An article by Tunick et al. retrospectively described the outcome of 519 patients with severe aortic plaque on transoesophageal echocardiography, treated with statins, warfarin or antiplatelet medication. In this study the atheroemboli syndrome occurred in five patients, where only two patients were taking warfarin.18 Furthermore, an article published in 1987 described a review of 221 cases from the literature with histologically proven cholesterol crystal embolisation. The possible predisposing factor of the use of anticoagulants was reported in 30 patients.19
A postulated mechanism on how anticoagulants may induce cholesterol embolisms is by inducing haemorrhage in an atheromatous plaque, or by dissolution of the fibrous cap around the atheromatous core, resulting in the release of cholesterol in the systemic circulation.13
Because cholesterol crystal embolisms can occur spontaneously, a coincidental effect of starting a DOAC and spontaneous cholesterol crystal embolisation in the described cases cannot be ruled out, but the time relationships after start of the DOAC in the described cases, supported by a possible mechanism, indicate a possible causal relationship between treatment with a DOAC and cholesterol crystal embolisation.
It is important to realise that when a patient develops cholesterol crystal embolisms while on therapy with a DOAC, this may concern an adverse drug reaction of the DOAC.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
DISCLAIMER
The authors are indebted to the national pharmacovigilance centres that contributed data to the EudraVigilance database, maintained by the European Medicines Agency EMA. The opinions and conclusions, however, are not those of the various centres, nor of the EMA. The information originates from a variety of sources, and the likelihood that the suspected adverse reaction is drug related can vary between cases.
REFERENCES