KEYWORDS
Intestinal ischaemia, L-lactate, D-lactate
INTRODUCTION
One of the possible causes of severe abdominal pain is acute mesenteric ischaemia (AMI), a life-threatening disease with a high mortality rate. The in-hospital mortality is around 60%.1 Based on aetiology there are four types of AMI. Most frequently, accountable for approximately 40-50% of the cases, AMI is caused by an arterial embolism from the heart or proximal aorta. In 25-30% of the cases AMI is caused by arterial thrombosis in an atherosclerotic splanchnic artery. Non-occlusive mesenteric ischaemia is responsible for approximately 20% of the mesenteric ischaemic events which may for example be due to hypovolaemia, as systemic vasoconstriction induces splanchnic hypoperfusion. Finally, the least common type is mesenteric venous thrombosis which occurs in around 10% of the patients.2
The high mortality rate is largely caused by diagnostic delay in this fast-progressing disease,3 although significant comorbidity in patients with AMI also plays a role. Clinical symptoms such as pain often do not correlate with other clinical signs, such as signs of peritonitis.4,5 Therefore the need for a reliable and accurate diagnostic test is high. Prior to imaging, many clinics measure the serum lactate concentration as part of the diagnostic work-up for the diagnosis of intestinal ischaemia.
There are two different isomers of lactate: D-lactate and L-lactate. L-lactate is the end product of anaerobic glycolysis. During this process it is formed out of pyruvic acid by the enzyme lactate dehydrogenase (LDH). During ischaemia and also intestinal ischaemia, the cells will start anaerobic dissimilation and the serum lactate rises.6 Next, L-lactate is absorbed, mostly by the liver but partially by the kidney. There it is converted back to pyruvate and by gluconeogenesis to glucose. Thus, an increased serum L-lactate can be a result of tissue hypoperfusion, as well as a decreased lactate metabolism in the liver or kidney. Furthermore various other medical conditions are associated with an increase in serum L-lactate, such as diabetic keto-acidosis and malignancy.6 Experimental studies have shown that the liver is able to increase lactate uptake in case of excessive mesenteric lactate production so that an increased serum L-lactate can be compensated.7 D-lactate is an isomer of lactate that is not produced by the human body, but released by intestinal bacteria. Increased serum D-lactate during intestinal ischaemia might be caused by bacterial overgrowth of these bacteria.6 The D-isomer is metabolised by a D-LDH enzyme.6 In daily care, lactate measurement includes L-lactate, which is measured by using an enzymatic reaction between L-lactate and either L-lactate oxidase or L-LDH. Both of these enzymes are specific for L-lactate. Therefore, D-lactate is not routinely obtained when measuring L-lactate. D-lactate is measured by using an enzymatic reaction with D-LDH, which is not available in most hospitals.
The goal of this review is to assess the diagnostic value of serum L-Lactate and D-lactate measurement in acute mesenteric ischaemia, and thereby ascertain whether or not these should be used in daily practice. 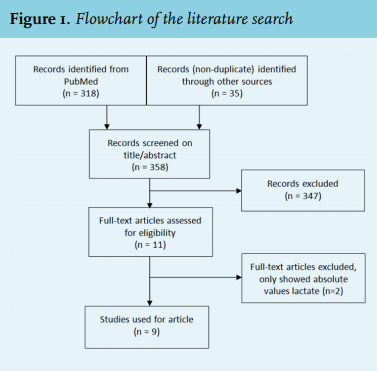
METHODS
To find available literature on serum lactate measurement we performed a literature search in PubMed, Cochrane and Embase with the search terms lactate, lactic acid, marker, mesenteric, intestinal, bowel, colon, colitis, ischaemic, ischaemia, infarction and their corresponding MeSH terms. The search was limited to English full-text articles conducted in humans. Results of the search are shown in figure 1.
Studies, (systematic) reviews or meta-analyses about the diagnostic value of lactate or multiple biomarkers including lactate were included. Exclusion criteria were case reports and articles about mesenteric ischaemia after a specific type of surgery. To find additional literature not discussed in reviews or not found by the search, Web of Science was used for a cross-reference search. We found 358 unique articles, which were screened on title and abstract. Eleven full-text articles were assessed for their eligibility, of which two articles were excluded as they only compared absolute values of lactate between patients with and without AMI, and did not assess the diagnostic value.
If the sensitivity or specificity of the test was not given and sufficient data were available, we calculated these parameters according to standard methods.
RESULTS
L-lactate in acute mesenteric ischaemia
In a review in 2012, Demir et al.6 described six relatively small studies on the diagnostic value of L-lactate for acute mesenteric ischaemia, with variable results (table 1).8-14 The three oldest studies show a high sensitivity for acute mesenteric ischaemia of over 90%, whereas the three more recent studies show a low to moderate sensitivity (total range sensitivity 33%-100%). For several reasons, these results should be interpreted with caution. First, in two of the three studies with a high sensitivity, lactate was partially obtained preoperatively and not during initial evaluation while in some cases there was a significant time interval between initial evaluation and surgery.8,9 In the study conducted by Lange et al.8 sensitivity was 100%, but the median symptom duration was 43 hours and the postoperative 30-day mortality was 90%. Second, two of the three studies reporting a high sensitivity may have an overlap in patient cohort as both were conducted by the same author.8,10 One of the three studies with low sensitivity included patients with mechanical bowel obstruction, and only three patients with gut necrosis.12 Since two of the six studies included patients with AMI retrospectively, the specificity was not calculated in these studies. In the remaining four studies there was a low specificity (range 36%-72%). In view of these data, the use of serum L-lactate measurement in our opinion appears to be unfit for the diagnosis of AMI since in general it has a low specificity and a moderate sensitivity. 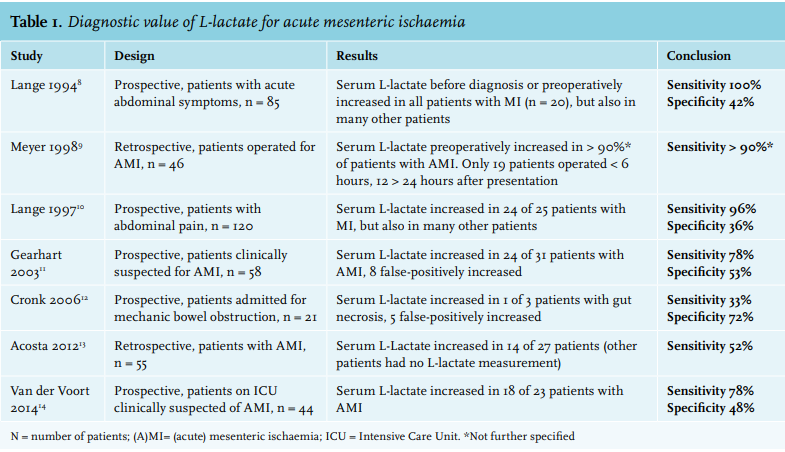
The prognostic value of L-lactate in intestinal ischaemia
Although the usefulness of L-lactate as a diagnostic marker is limited, it still might have a prognostic value. In a retrospective French study of patients with AMI admitted to the intensive care unit (ICU), a serum L-lactate > 2.7 mmol/l gave an odds ratio (OR) for ICU mortality of 2.36 (95% CI 1.52-3.66) in a multivariable analysis.15 A similar result was found in another study with patients operated for AMI, where the mortality was significantly increased in patients with a serum L-lactate above 2.0 mmol/l (p < 0.002, no OR, univariate analysis).16 These studies show that an increased serum L-lactate appears to be an unfavourable prognostic sign rather than a diagnostic marker for AMI.
D-lactate in acute mesenteric ischaemia
A systematic review by Evenett et al.4 discussed multiple serological markers for intestinal ischaemia and included a review of four studies on D-lactate. Since two of those four studies were conducted in patients after aorta surgery, we do not present these. In the two other studies, D-lactate was measured prospectively in patients with acute abdominal complaints (table 2). One of the studies obtained the D-lactate preoperatively. This study found a high sensitivity and specificity. The other study, which measured D-Lactate at presentation of symptoms, showed a high sensitivity but a very low specificity of 23%.17,18 In a comparable cohort from a recent Chinese prospective trial, sensitivity was moderate at 67% but specificity was high (86%).19 Although D-lactate appears to be a little bit more reliable than L-lactate as a diagnostic marker for AMI, its performance in the current literature is still not good enough to be used in daily practice. 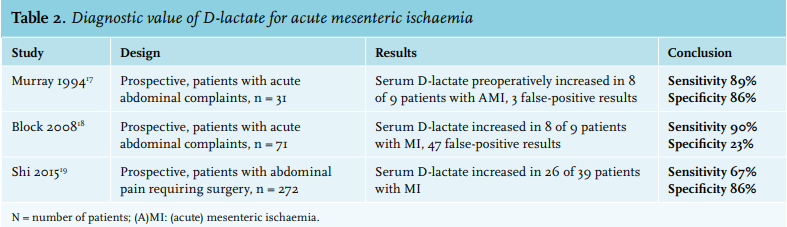
DISCUSSION
Acute mesenteric ischaemia is a rapidly progressive disease with high mortality. Whereas the current European Society of Vascular Surgery (ESVS) guideline for vascular mesenteric disease advises to perform CT angiography in patients with high clinical suspicion,20 L-lactate is often incorporated in the diagnostic work-up in daily clinical practice. Obviously, the need for a reliable biomarker is high, as it can increase clinical suspicion for AMI and thus reduce delay.1 The routinely measured serum L-lactate, however, does not seem to be the appropriate candidate.
Although the sensitivity of the test was high in some older studies, these studies had severe methodological limitations.8-10 Newer studies found a much lower sensitivity, making serum L-lactate an unfit test in ruling out AMI.11-14 Moreover, all studies found a low to moderate specificity, corresponding to the fact that there are many other causes for a high serum L-lactate. In our opinion, L-lactate should not be used to diagnose or rule out acute occlusive mesenteric ischaemia. This view is shared by the recent ESVS guideline for vascular mesenteric disease.20 While the diagnostic value of L-lactate is limited, other studies showed that it might have a role as a prognostic marker, since patients with a high serum L-lactate demonstrate an increased mortality rate. The most probable explanation seems to be that an increased serum L-lactate in AMI reflects advanced AMI.15,16
The sparingly measured isomer D-lactate also appears to be too unreliable for the diagnosis of AMI. A study where serum D-lactate was obtained preoperatively showed promising results, but the studies where serum D-lactate was obtained at initial presentation of the patient did not demonstrate added value of the test.17-19 Possible explanations for the limited value, despite the exclusive intestinal origin of D-lactate, are that increased serum D-lactate values are also found in people with a high carbohydrate intake, people who use probiotics and those who have decreased colon motility.6 Other studies have found that serum D-lactate levels are elevated in people who have had a jejunoileal bypass operation or who have the short-bowel syndrome.17
Although serum D-lactate in general performed slightly better than serum L-lactate, the results are inconsistent. Moreover, there were not many studies investigating D-lactate and regrettably not a single study compared serum D- and L-lactate in a single study population. Although Van der Voort et al.14 looked at both tests in their ICU study, they only presented absolute values for D-lactate and no sensitivity or specificity. It is therefore impossible to compare the diagnostic performance of the two isomers in this study group.
Though not readily available in daily practice, the measurement of intestinal fatty-acid binding proteins (i-FABP) might have diagnostic value in intestinal ischaemia. These proteins are located in the enterocyte and help with the transport of fatty acids over the cell membrane. When mucosal damage occurs, these proteins enter the circulation and are detectable.5,19,21,22 Multiple prospective trials have recently been conducted to assess the diagnostic value of i-FABP in mesenteric ischaemia. In a meta-analysis published in 2016 the results of the diagnostic value of i-FABP from nine studies were pooled, resulting in a pooled sensitivity of 0.80 (95% CI: 0.72-0.86) and a pooled specificity of 0.85 (95% CI: 0.73-0.93).21
In the three biggest trials, especially the negative predictive value (NPV) stood out. Although the NPV is specific for a certain patient population and not for the test itself, it was remarkably high in all three populations. In a Japanese trial where small bowel ischaemia was found 52 times in 361 patients with acute abdomen, the NPV of i-FABP was 95%.22 An NPV of 96% was found in a Chinese trial with 272 patients with abdominal pain requiring surgery where 39 had mesenteric ischaemia.19 Another Japanese trial where 24 cases of AMI were found in 208 patients clinically suspected for AMI, showed an NPV of 98%.5 The positive predictive value (PPV) of the serum i-FABP test was very low in these studies, 32%, 33% and 50%, respectively.5,19,22 Thus, although the potential to diagnose AMI is very limited, it might be very useful in virtually excluding the diagnosis of AMI. Currently an ELISA method is used for the serum i-FABP measurement. Since this test takes three to four hours, its clinical use is limited.19,22 However, Kanda et al.22 report that they are developing a faster test (< 1 hour). Although, in the currently available literature, the D-dimer test too has a very poor specificity,4 the sensitivity is around 95% in multiple studies.20 The ESVS therefore now recommends a D-dimer test to exclude AMI in patients with acute abdominal pain.20
Besides the two isomers of lactate and i-FABP, many other biomarkers were also investigated for their diagnostic value regarding AMI. For instance, creatine kinase, leukocyte count, C-reactive protein and LDH showed inferior results compared with lactate.4,19 Multiple reasons have been put forward in the literature as to why finding a reliable biomarker for intestinal ischaemia appears to be this hard. First, the release of intestinal proteins into circulation might not start until severe mucosal damage has occurred. Second, the blood collected in the intestine passes the liver first, which might prevent these proteins from entering the systemic circulation.17 Finally, non-occlusive mesenteric ischaemia is often present in ICU patients.23 These patients are often included as control group in studies assessing biomarkers for AMI, which obviously hampers the discriminative power as a marker of AMI.
CONCLUSION
Acute mesenteric ischaemia (AMI) is a life-threatening disease with a mortality rate around 60%. This high mortality rate is largely caused by diagnostic delay. Diagnosis is made by CT angiography with a slice thickness of 1 mm or thinner. A reliable biomarker is needed for early diagnosis and for the ability to correctly assess a patient’s likelihood of ischaemia to increase clinical suspicion and thereby reduce delay. Although frequently measured in daily practice, as part of the diagnostic work up, L-lactate appears to be unsuitable to be used due to its low specificity and moderate sensitivity. Instead, an increased serum L-lactate in AMI is in general an unfavourable prognostic sign indicating an increase of mortality risk.
DISCLOSURES
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES