KEYWORDS
Angiomatosis, benign mediastinal tumour, mediastinal angiomatosis, mediastinal tumour, mediastinum
CASE 1
A 34-year-old woman presented with a swelling above the left clavicle. Magnetic resonance imaging (MRI) showed a mass extending from the left upper mediastinum to the left supraclavicular area, measuring 6 cm in the largest diameter. Left thoracotomy was performed which revealed a mass that infiltrated within the pectoral muscle fibres, infiltrating the pericardium and extending behind the left clavicle. The tumour was completely resected. Macroscopic examination revealed a fatty appearing mass with multiple blood vessels and haemorrhagic foci. Histologically, the lesion was composed of mature fat tissue and randomly scattered multiplied, irregular, dilated blood vessels, with thick walls, predominantly of the venous type. Clusters of capillary-sized vessels were adjacent to larger vessels and in their walls. The lesion was deemed to be angiomatosis. The patient was followed up with chest X rays at 1, 3 and 6 months postoperatively. There were no signs of recurrence of the disease 10 months after surgery. 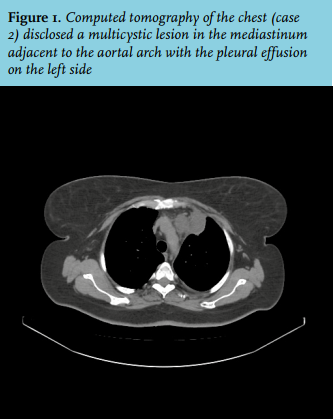
CASE 2
A 57-year-old woman presented with dyspnoea, general weakness and a left-sided pleural effusion of 2 months’ duration. She had a previous history of cholecystectomy, bilateral adnexectomy due to endometriosis and a 10-year history of treated hypertension. Computed tomography of the chest disclosed an infiltrative mass in the mediastinum with the left-sided pleural effusion (figure 1). Video-assisted thoracoscopic surgery was performed in another institution and was unsuccessful. A positron emission tomographycomputed tomography scan performed afterwards revealed minimal metabolic activity (maximum standardised uptake value was 2.7). No pathological findings were seen in the regional lymph nodes and the biodistribution of the glucose analogue in the rest of the body was normal. An open thoracotomy was performed during which a mediastinal tumour was found. It extended above the aortic arch, infiltrating the brachiocephalic vein, and vagal and phrenic nerve. The tumour and infiltrated structures were completely resected. Macroscopic examination showed a yellow mass with multiple blood vessels and poorly defined borders measuring 4 x 3 x 1.5 cm. The lesion was similar to the lesion described in the first case, and diagnosed as angiomatosis. The pleural effusion cyto-analysis showed a lymphocytic type of effusion (80% lymphocytes, 15% mesothelial cells, 5% macrophages) and no trace of malignant cells. Her follow-up was at 1, 3, 6 months postoperatively with no signs of local recurrence on the CT scan 10 months after the operation (figure 2A and B). 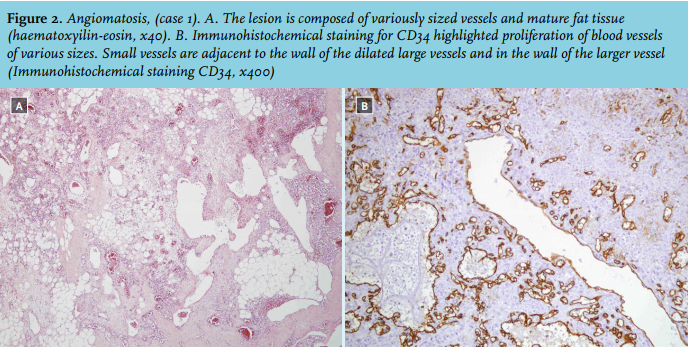
DISCUSSION
Angiomatosis is a rare benign vascular lesion with extensive and infiltrative growth. It is usually found in the lower extremities, followed by the chest wall, abdomen and upper extremities. Angiomatosis located in the mediastinum is extremely rare, especially when found as a solitary lesion, as in the two cases presented here.
It is assumed that angiomatosis has its inception in utero or in the neonatal period given its slow growth. This could explain why angiomatosis usually gives rise to its first symptoms in the first two decades of life.1 We have shown two rare cases of mediastinal angiomatosis with a late onset in two female patients. Our 57-year-old patient is the second oldest reported patient with newly discovered mediastinal angiomatosis (the oldest reported patient was 63 years old).2
On the CT and MRI, angiomatosis shown as a diffuse nonhomogeneous mass can give a mistaken impression of a malignant tumour. Macroscopically seen serpiginous density within this mass (the areas histologically correspond to tortuous vessels) can point to angiomatosis, but the final diagnosis is usually established by histology.3 The histological characteristic of angiomatosis is mature fat tissue and large irregular veins along with capillary-sized vessels adjacent to or in their walls,1 as was found in the cases described here. Angiomatosis is histologically different from infiltrating lipoma, angiolipoma, angiomyolipoma, angiomyxolipoma, intramuscular angioma and liposarcoma,1 which can macroscopically look similar.
Patients with mediastinal angiomatosis usually present with symptoms of haemorrhage (haemothorax, haemomediastinum, haemoptysis),4 local compression (dyspnoea, cough),3 chest pain and pleural effusion,2 although sometimes these lesions are incidentally detected.5 Similarly to those reported symptoms, one of our patients presented with pleural effusion and the other one with neck swelling.
In localised cases of angiomatosis, complete surgical resection is the treatment of choice because of the high tendency for local recurrence.1 In the study reported by Rao et al.,1 50% of patients with angiomatosis in various anatomical locations had local recurrences. That is probably due to the incomplete excision of the lesions (according to the authors, 90% of these lesions persisted after surgical excision). In their study, recurrences usually occurred within five years after excision. No data were found specifically for mediastinal angiomatosis. None of the seven cases of mediastinal angiomatosis found in the PubMed search reported recurrence. The longest reported follow-up was 14 months.5 Hence further, long-term follow-up of patients with mediastinal angiomatosis is necessary.
There are no current guidelines for the treatment of angiomatosis. Though angiomatosis does not show a tendency for malignant alteration, due to its infiltrative and extensive growth, it can cause significant clinical complications. It is important to recognise angiomatosis, treat it with wide surgical excision and monitor with close follow-up.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES