KEYWORDS
Blood pressure, lipids, obesity, epidemiology, treatment
INTRODUCTION
Several long-term follow-up studies have shown that cardiovascular risk gradually increases with increasing levels of blood pressure (BP) and low-density lipoprotein cholesterol (LDL-C).1-3 Current risk engines and guidelines give specific estimates of excess of risk related to these risk factors.4-8 They also describe target levels for BP and LDL-C above which pharmacotherapy should be started or intensified.
As the BP rises with increasing age, setting a specific target level for treatment may be appropriate for a younger age group, but too aggressive for an elderly age group. Indeed, there may be considerable side effects of aggressive BP-lowering treatment in the elderly.9,10 In the Joint National Committee (JNC) 8 treatment guideline for hypertension, it was advised to aim for a BP < 140/90 mmHg in non-diabetic adults (< 60 years), whereas BP values < 150/90 mmHg were advised for elderly people (≥ 60 years). However, the recent SPRINT study suggested that a systolic BP in the 125-135 mmHg range is probably the optimal target for most hypertensive patients.11
Elevated LDL-C levels have been identified as another major factor contributing to cardiovascular disease (CVD). A multitude of randomised clinical trials have shown that cholesterol lowering with statin therapy reduces cardiovascular morbidity and mortality.12,13 The 2011 ESC/ EAS Guidelines for the management of dyslipidaemias proposed an LDL-C treatment target of < 2.5 mmol/l for subjects at high risk, while for subjects at moderate risk, an LDL-C target of < 3.0 mmol/l could be considered.5
Obesity is a major contributor to the global burden of chronic diseases and disabilities.14,15 Increased adiposity is a key risk factor for hypertension, dyslipidaemia, type 2 diabetes and cardiovascular disease. Previously, we have shown that elevated BP ≥ 140 mmHg was present in 45-70% of obese individuals in an international multi-cohort study.15 In the NHANES study, prevalence of hypertension and dyslipidaemia was the highest in obese participants compared with overweight and non-obese individuals.16
Several studies have reported on the quality of BP and lipid control in several distinct populations,17-18 as well as measures to enhance medication adherence.19 In 2014, data from NHANES showed that untreated hypertension had decreased among obese and overweight adults and untreated dyslipidaemia had decreased for all weight groups.16 The recent EUROASPIRE IV survey showed, however, that large proportions of patients at high CVD risk have insufficiently controlled BP and lipids.20 Other recent papers have suggested a degree of clinical inertia in treating high BP, especially in the context of obesity.21,22
In this paper we report cross-sectional data on levels of BP and LDL-C, and treatment of these risk factors in participants of the Lifelines Cohort Study, a prospective population-based study in the Netherlands. The analysis is part of a ‘Healthy Obesity’ research program.15 The main question we aimed to answer was whether there were differences in the cardiovascular risk factor levels of BP and LDL-C for obese subjects within different age cohorts compared with those with normal weight and overweight. Also, we wanted to assess the quality of single and combined treatment of BP and LDL-C in these subjects.
MATERIALS AND METHODS
Subjects
In this cross-sectional study, we used data from subjects participating in the Lifelines Cohort Study. Lifelines is a multi-disciplinary prospective population-based cohort study examining, in a unique three-generation design, the health and health-related behaviours of persons living in the north of the Netherlands. It started in 2007, and employs a broad range of investigative procedures in assessing the biomedical, socio-demographic, behavioural, physical and psychological factors which contribute to the health and disease of the general population, with a special focus on multi-morbidity and complex genetics. The methodology has been described previously.23,24 All participants were between 18 and 90 years at the time of enrolment. They provided written informed consent before participating in the study. The study protocol was approved by the medical ethics review committee of the University Medical Center Groningen. In the present study, we included subjects with an age between 18 and 80 years, who were of Western European descent, did not have diabetes mellitus, and who participated between 2007 and 2013.
Clinical examination and definitions
Subjects completed a self-administered questionnaire on medical history, past and current diseases, use of medication and health behaviour at home. Medication use was verified by a certified research assistant, and scored by the Anatomical Therapeutic Chemical (ATC) Classification System, a system developed for the classification of active ingredients of drugs. The number of different medications used by a participant was considered a proxy for multimorbidity.25 Diagnosis of type 2 diabetes mellitus was based either on self-report (known diabetes), or on the finding of a single measurement of fasting blood glucose ≥ 7.0 mmol/l at Lifelines’ screening (newly-diagnosed diabetes). Smoking status was defined as non-smoker, former smoker and current smoker (including the use of cigarettes, cigarillos, cigars and pipe tobacco).
A standardised protocol was used to obtain BP and anthropometric measurements: height, weight, and waist circumference. BP was measured every minute during a period of 10 minutes with an automated DINAMAP Monitor (GE Healthcare, Freiburg, Germany). The size of the cuff was chosen according to the arm circumference of the participant. The average of the final three readings was recorded for systolic and diastolic BP. Because of the great interest for systolic BP control in the prevention of CVD, in this paper we focus on systolic BP only. Heart rate was measured simultaneously with the BP. Anthropometric measurements were done with the participant in light clothing and without shoes. Body weight was measured to the nearest 0.1 kg. Height and waist circumference were measured to the nearest 0.5 cm. Waist circumference was measured in standing position with a tape measure all around the body, midway between the lower rib margin and the iliac crest. Body weight and height were used to calculate body mass index (BMI) (weight (kg)/height (m)2 ), which was categorised as normal weight (18-25 kg/ m2 ), overweight (25-30 kg/m2 ) and obesity (≥ 30 kg/m2 ). As many of the Lifelines participants are treated solely by their general practitioner, we applied the target and cut-off values for high BP (< 140 mmHg) and elevated LDL-C (< 2.5 mmol/l) valid in 2013.
Biochemical measurements
Blood samples were collected in the morning after an overnight fast, directly into tubes containing heparin, and centrifuged. Serum levels of total and HDL cholesterol were measured using an enzymatic colorimetric method, triglycerides using a colorimetric UV method, and LDL-C using an enzymatic method, all on a Roche Modular P chemistry analyser (Roche, Basel, Switzerland). Serum creatinine was measured on a Roche Modular P chemistry analyser (Roche, Basel, Switzerland). Fasting blood glucose was measured using a hexokinase method.
Calculations and statistical analysis
BP and LDL-C are reported in subgroups that were defined by sex, BMI (normal weight, overweight and obese) and age groups (18-30 years, 30-40 years, 40-50 years, 50-60 years, 60-70 years and 70-80 years), and -if applicable- treatment status. Diagnosis of metabolic syndrome was established if a subject satisfied at least three out of five criteria according to the modified guidelines of the National Cholesterol Education Programs Adults Treatment Panel III (NCEP ATPIII criteria): (1) systolic BP ≥ 130 mmHg and/or diastolic BP ≥ 85 mmHg and/or use of antihypertensive medication; (2) HDL cholesterol levels < 1.03 mmol/l in men and < 1.30 mmol/l in women and/or use of lipid-lowering medication influencing HDL levels; (3) triglyceride levels ≥ 1.70 mmol/l and/or use of triglyceride-lowering medication; (4) waist circumference ≥ 102 cm in men and ≥ 88 cm in women; (5) fasting glucose level ≥ 5.6 and/or use of blood glucose-lowering medication and/or diagnosis of type 2 diabetes.26 Coronary artery disease was defined when subjects reported any of the following diseases: myocardial infarction, percutaneous coronary intervention, or coronary artery bypass grafting.
All analyses were conducted using PASW Statistics (Version 24, IBM, Armonk, NY, USA). Data are presented as mean ± SD, or median and interquartile range when not normally distributed. Means were compared between groups with analysis of variance. When variables were not normally distributed, medians were compared with the nonparametric Kruskal-Wallis test. Chi-square test was used to analyse categorical variables. To adjust for multiple comparisons, a p-value < 0.01 was considered statistically significant.
RESULTS
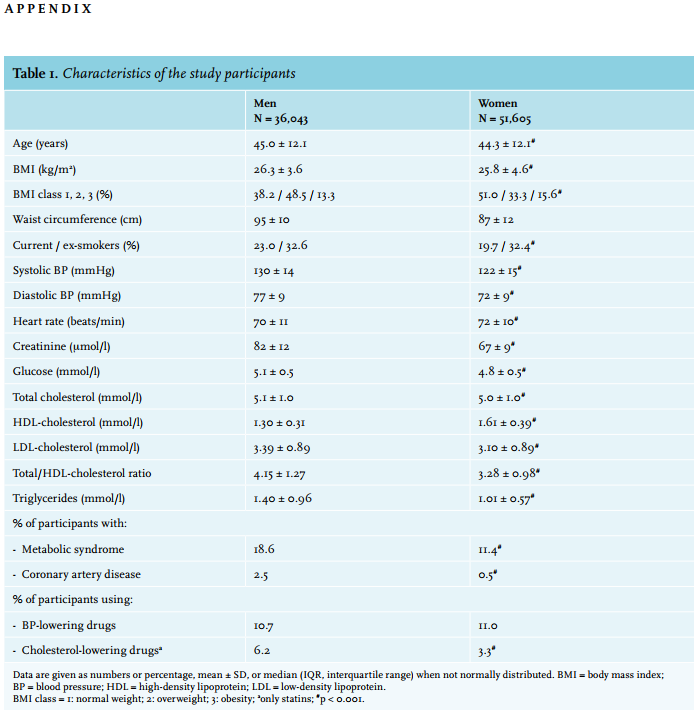
Participant characteristics are given in table 1 and in the Appendix, table 1. In total, data of 87,648 individuals were available for analysis.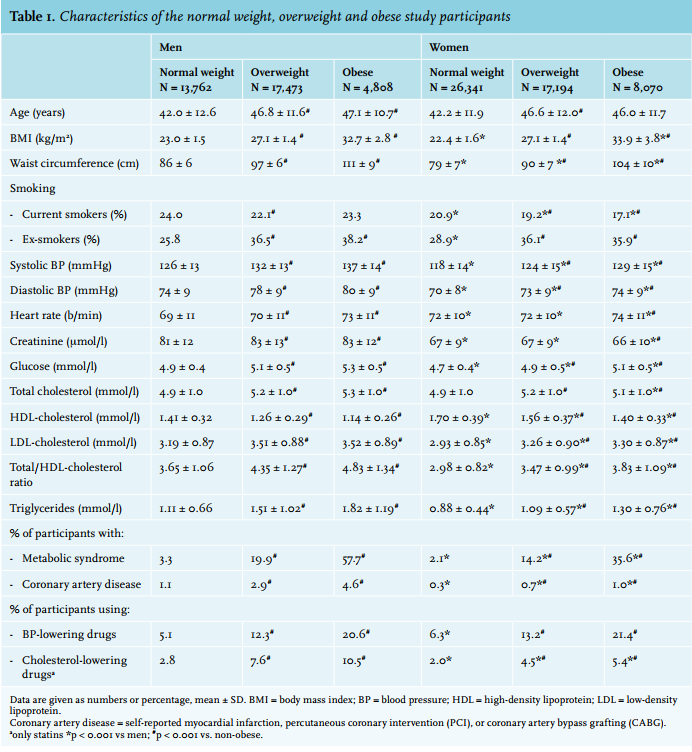
Clinical characteristics
Overall, women had a lower BP and generally more favourable lipid profiles, with lower LDL-C and triglyceride levels, and more women had a normal BMI than men. A similar percentage of men and women were treated with BP-lowering drugs, but fewer women used statins. In total, 10.8% of participants were using BP-lowering drugs, and 1.6% used more than two types of BP-lowering medication. In comparison with normal weight individuals, overweight and obese people had higher levels of BP, heart rate, glucose and lipid levels. More overweight and obese participants were treated with BP-lowering drugs and statins. For each BMI class, women had lower levels of BP, creatinine, LDL-C and triglycerides, and higher levels of HDL-C compared with men. Fewer women than men were current smokers, and used cholesterol-lowering drugs.
Effects of age and treatment on BP
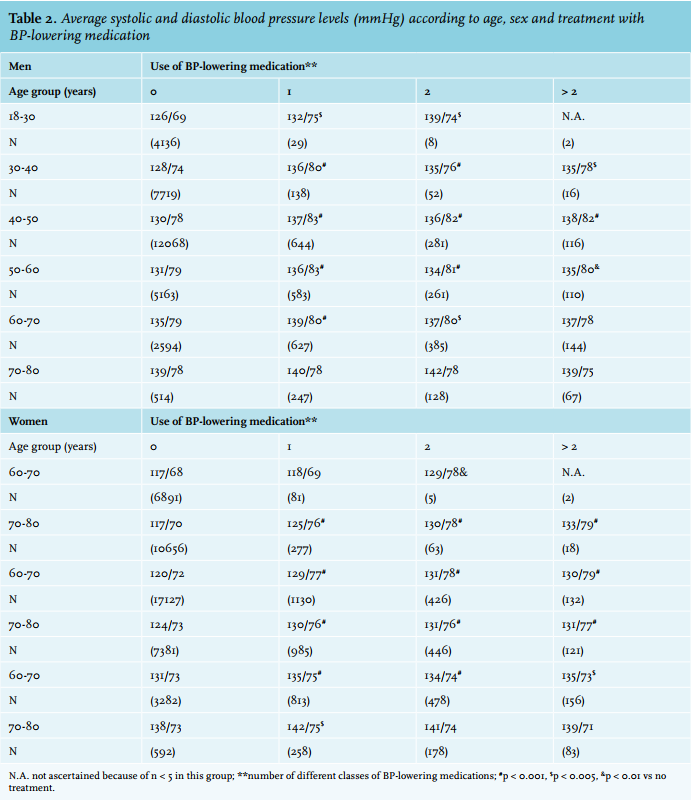
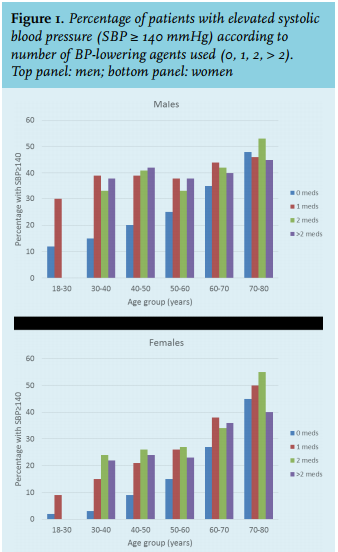
In those not using BP-lowering drugs, the BP increased gradually in each age group, with mean levels of 126/69 mmHg in men and 117/68 mmHg in women aged 18-30 years, which gradually increased with higher age to levels of 139/78 mmHg in men and 138/73 in women aged 70-80 years (Appendix, table 2). In general, participants using BP-lowering drugs still had higher BP levels compared with individuals not using BP-lowering drugs, except in the male participants over the age of 60, and female participants aged 70-80 years. The largest difference in BP between treated and not-treated individuals amounted to 13/5 mmHg in the youngest males, and 13/10 mmHg in the youngest female group using two BP-lowering drugs (both p < 0.001). Appendix, figure 1 depicts the percentage of individuals, stratified for age, who had elevated systolic BP ≥ 140 mmHg in each of the medication groups. Despite the use of BP-lowering medication(s), still a significant number of participants had insufficiently controlled BP: 30-50% of men and 20-50% of women do not achieve the desired target levels of systolic BP < 140 mmHg. In the participants not using BP-lowering drugs, especially in those over the age of 50 years, still 14-45% would be eligible for treatment based on a BP level ≥ 140 mmHg. The figure also shows that fewer women than men have elevated BP ≥ 140 mmHg.
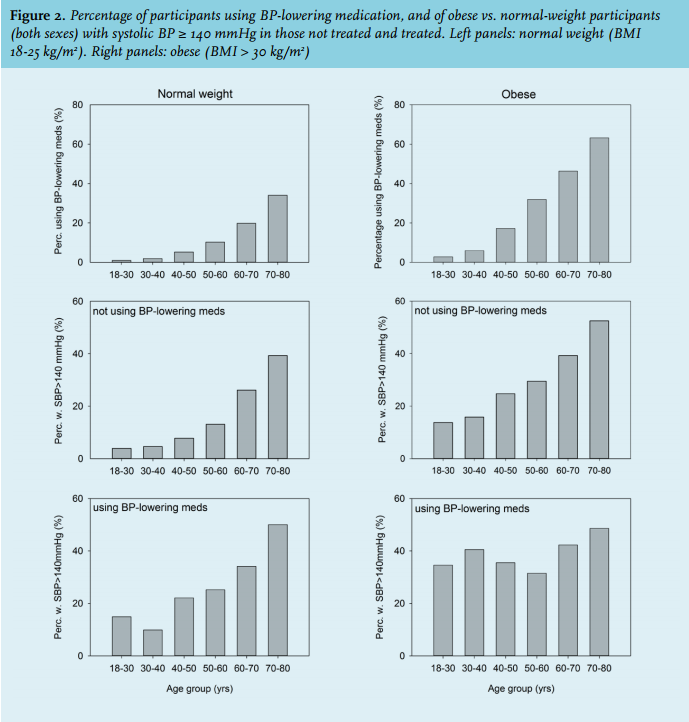
BP: obesity vs. normal weight and overweight
Next, we analysed differences in BP according to the level of BMI (figures 1A and 1B). BP levels were significantly higher in all age groups in obese vs. normal weight and overweight individuals, in both men and women. This difference was the largest in the youngest age group (+11 mmHg in obese men, p < 0.001 vs. overweight and normal weight). In normal weight and overweight men and women, there was a clear difference in BP levels for all age groups (except the 70-80 year group) between untreated and treated individuals. This was less apparent in the obese. It should be noted that the use of BP-lowering medications was much higher in obese participants (figure 2). Despite this, a larger percentage of obese individuals had elevated systolic BP ≥ 140 mmHg (treated and untreated). Depending on the age group, 14% in the youngest and 52% in the oldest obese participants were not treated with BP-lowering medication, while for normal weight individuals this varied between 4% and 39% (figure 2). For obese participants treated with BP-lowering drugs, 35% in the lowest age group and 49% in the highest age group had systolic BP ≥ 140 mmHg. For normal weight participants these percentages were 15% and 50%, respectively.
LDL-cholesterol: obesity vs. normal weight
Overall mean LDL-C was 3.52 ± 0.89 mmol/l in obese vs. 3.19 ± 0.87 mmol/l in normal weight men (p < 0.001), and 3.30 ± 0.87 vs. 2.93 ± 0.85 mmol/l in normal weight women (p < 0.001). Overweight participants had an LDL-C similar to those who were obese. In men, overall 6.2% were using statins, which was 0.3% in the youngest age group and 27% in the oldest age group. In addition, 10.5% of obese men vs. 2.8% of normal weight and 7.6% of overweight men were using a statin (p < 0.001). In women, overall statin use was 3.3%, with 0.2% in the youngest age group and 20% in the oldest age group, respectively. More obese women were using statins than those with normal weight (5.4% vs. 2.0%, p < 0.001).
Figure 3 shows that LDL-C levels increased with age in both sexes, with higher levels in obese vs. normal weight individuals at all ages, while it remained at a constant level in those using statins. As can be seen, mean LDL-C levels varied between 2.5 and 3.0 mmol/l in men and women using statins. The overall number of statin users reaching an LDL-C target < 2.5 mmol/l was 37% in men and 29% in women. More untreated obese than normal weight participants had an LDL-C ≥ 3.5 mmol/l (men: 56% vs 37%, women: 41% vs 24%, both p < 0.001). 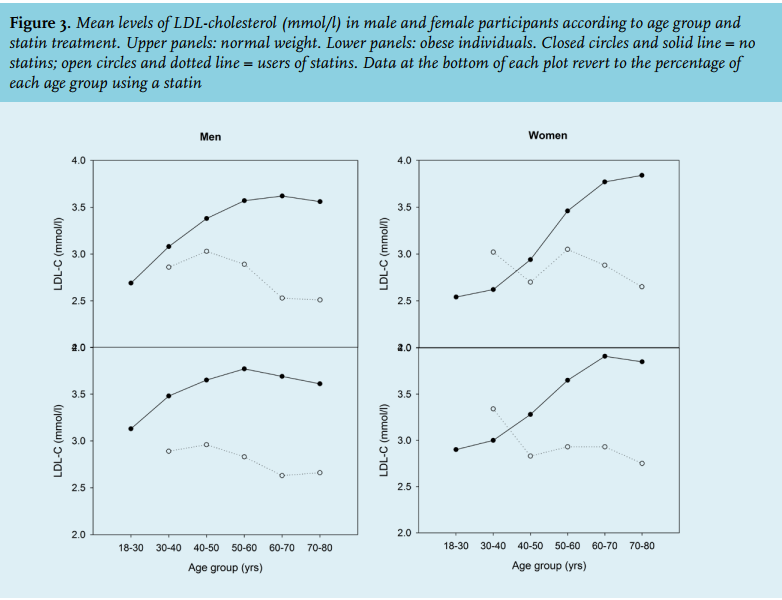
Combined risk factor treatment
Finally, we assessed lipid treatment and its levels in relationship to BP medication (combined risk factor intervention). There were slight differences of combined BP-lowering and statin treatment according to BMI. In normal weight, overweight and obese men treated with BP-lowering medication, 26%, 33% and 33% were also using statins; in women, these percentages were significantly lower, i.e. 15%, 20% and 16%, respectively.
DISCUSSION
We found that in people of Western-European descent, obese individuals of both sexes have a higher BP and LDL-C compared with overweight and normal weight individuals, and especially obese men younger than 50 years have elevated BP levels. Use of BP-lowering drugs does not revert BP back to levels normal for the specific age group, and 10-50% of individuals in the various age groups do not achieve the desired target levels of systolic BP < 140 mmHg. Although cholesterol-lowering statins abolish the age-related increase in LDL-cholesterol in both men and women, the majority do not reach the target level of < 2.5 mmol/l.
The changes of BP levels with ageing were compared between individuals not using BP-lowering medications, and those who were treated with these drugs. Due to the large number of participants, we were able to stratify not only for sex, age and BMI, but also for the number of different BP-lowering medications used. We clearly demonstrated an age-dependent increase of BP, and significantly higher BP levels in men compared with women. In the participants not using BP-lowering drugs, especially in those over the age of 50 years, still up to 45% would be eligible for treatment based on a BP level ≥ 140 mmHg. In addition, despite treatment with one or more BP-lowering drugs, 30-50% of men and 20-50% of women do not achieve the desired target levels of systolic BP < 140 mmHg. This has also been reported in earlier cohort studies, for instance the German population-based cohort SHIP,27 the Hispanic Community Health Study28 and a study in rural Australia,29 which clearly showed that the proportion of participants receiving therapy and the number of participants reaching their target BP values were insufficient. Similar observations have been reported in diabetic individuals.30,31 Very recent data from the EPIC prospective cohort study confirmed that, amongst others, overweight, obesity, and hypertension contributed significantly to premature death.32
We used a cut-off level of 140 mmHg, as current guidelines advise to start treatment at a systolic BP ≥ 140 mmHg, and to lower until systolic BP levels < 140 mmHg have been reached.5 The use of this BP goal is likely to explain why many participants do not reach BP levels which are ‘physiological’ for their age. This difference between ‘normalisation’ of BP vs. ‘achieving treatment targets’ may be of clinical relevance, as there may be additional cardiovascular benefit from more aggressive BP-lowering treatment. There are several studies which support this concept, as summarised by Ettehad et al.,33 who suggested that lowering BP to systolic levels < 130 mmHg may be feasible and beneficial. As an example, the Hypertension Optimal Treatment (HOT) study showed that the optimal target for cardiovascular protection was in the range 80-85 mmHg for diastolic BP and in the range 130-140 mmHg for systolic BP, and especially people with diabetes seemed to benefit from further BP reduction.34 However, there are indications that in some groups of patients, especially elderly people, this risk of aggressive BP-lowering may offset the benefits due to the so-called J-curve.35
We found a clear BP difference between men and women. Despite this, we observed that a similar percentage of both sexes were treated with BP-lowering medication. As we do not have any data regarding pre-treatment BP levels we can only speculate on the causes of these differences. It is apparent that fewer men reach treatment targets than women. This may be associated with a higher health consciousness in women, and the finding that women are more likely to visit their general practitioner than men.36 Of course, the BP values in the participants not using any medication depend on how often and rigorous GPs have been assessing them for high BP. In a situation where cardiovascular risk management is implemented fully, more people are screened, and therefore treated, for high BP.
Interestingly we found that the age-related increase in LDL-C was abolished by statin therapy and that contrary to BP-lowering medication, LDL-C levels are consistently lower in participants using statin treatment than those not using this medication. Mean LDL-C level on statin treatment varied between 2.5 and 3.0 mmol/l, indicating that a large number of participants did not reach the desired LDL-C level of < 2.5 mmol/l. Therefore, also these individuals can benefit from treatment intensification, for instance by switching from simvastatin to a more potent statin. However, we have to realise that LDL-C targets depend on integrated risk estimations,4-8 for which we do not have sufficient data in the individual participant.
At all ages, obese participants had higher levels of BP and LDL-C in comparison with overweight and normal weight participants. This is of clinical relevance, as people with a BMI above 30 kg/m2 clearly exhibit an increase in cardiovascular morbidity and mortality. Dudina et al. showed that obesity relates to CVD mortality in a strong and graded manner, especially in women and in younger persons.37 Earlier studies have also reported that BP increases with increasing waist-to-hip ratio.38 Obesity is a major contributor to chronic CVD and diabetes, and is also considered a key risk factor for hypertension. This applies to different countries, as a recent collaborative paper showed that elevated – and often untreated – BP ≥ 140 mmHg was present in 45-70% of obese individuals in an international study including cohorts from Germany, United Kingdom, Norway, Finland, Italy, Estonia and the Netherlands.15 Data from the NHANES study support this, and Saydah et al. reported that the prevalence of hypertension and dyslipidaemia was 35.7 and 49.7%, respectively, in obese participants.16 Although the same paper suggested that untreated hypertension and dyslipidaemia had decreased among obese adults,16 recent observations have indicated a degree of clinical inertia in treating high BP, especially in obesity.21,22 These recent papers are in contrast with a Dutch paper, which reported that obese men and women were more likely to consult their GP than persons without overweight, and more likely to receive drugs for the cardiovascular system.39 On the other hand, studies in the UK and in Finland reported that delays in initiation or intensification of BP-lowering therapy, or insufficient BP control per se, were associated with increased risk of an acute cardiovascular event or death.40,41
This study can perhaps also be considered a large-scale benchmarking of cardiovascular risk management in our country. An earlier paper by Klijs et al. already showed that, adjusted for differences in demographic composition, the Lifelines adult study population is broadly representative for the adult population of the north of the Netherlands.42 An important factor to consider in our results is the change of BP guidelines during the last decades. Treatment guidelines in 2003 and 2007 recommended a reduction of BP levels < 140/90 mmHg for uncomplicated hypertension and to < 130/80 for hypertension complicated by CVD, diabetes, or chronic kidney disease. In 2014 the JNC8 guidelines recommended less strict BP control, as a consequence of studies not showing any benefit of more aggressive BP control. In these guidelines, a cut-off of 150/90 mmHg for those over the age of 60 was proposed. The recent SPRINT study added new fuel to the debate, and suggested that a systolic BP in the 125-135 mmHg range is probably the optimal target for most hypertensive patients.11 SPRINT was the first study to show a benefit for further reduction of BP levels in people over the age of 75 years.43 However, it has been suggested that the unattended BP measurements performed in this study may corroborate with a 10 mmHg higher level in other studies.44
Strengths and limitations
Our study has some strengths and weaknesses. We have presented data for a large population-based study, in which all participants underwent careful examination, including structured and standardised BP measurements, and fasting LDL-C measurement in the same laboratory. Due to the large number of participants, we were able to stratify not only for sex, BMI and age group, but also for the number of different BP-lowering medications which were used by a participant. There are also a number of limitations. Measurements were performed at only one occasion, and physical examination was performed between 10 am and 6 pm. As a consequence, we could not control for possible diurnal variation of BP. Also, because of the cross-sectional nature, we only have information on current medication, and have no information on the response that a participant had exhibited earlier on the prescribed BP-lowering medication. Also, we did not have sufficient information to take statin dose into account.
Future directions
Large population-based studies such as Lifelines provide a lot of information on participants’ habits, medical treatment and comorbidities on one hand, and the results of cardiovascular risk management in general practice on the other hand.42 Studies such as this one would, however, immensely benefit from additional data obtained from the participants’ general practitioners, provided cardiovascular risk management and responses to earlier medical and nutritional interventions are carefully recorded and can easily be obtained for research purposes. In Lifelines, participants provided informed consent to obtain these data, but accessing them still poses major logistic and IT problems. Subsequent studies within Lifelines in which individual participants are interviewed about risk management and interventions may shed light on why people ‘escape’ cardiovascular screening programs. This also applies to better assessment of participants’ lifestyle and nutritional habits, for instance alcohol and salt consumption, both important factors in BP control. Adding this information may improve current screening practices and perhaps help more people to obtain treatment goals.
With regards to the differences between obese and normal weight and overweight individuals, more attention should be directed to active screening of obese individuals, and – as mentioned before – reducing clinical inertia in treating high BP, especially in obesity.21,22 A recent Dutch study on prescribing quality indicators reported that there is clear room for improvement in initiation and intensification of treatment of elevated glucose, lipids and BP for people with type 2 diabetes in primary care.45 This strongly agrees with the findings on BP in the current study. Future studies should evaluate new strategies for earlier recognition of treatable cardiovascular risk factors, especially in obese people, and ways to improve active invitation of obese individuals in screening and lifestyle intervention and – if deemed necessary – medical intervention to reduce the burden of obesity. We have observed a similar need for a more active approach regarding post-partum follow-up and lifestyle intervention in women with pregnancyinduced diabetes.46 Crucial for this are raised awareness and a more active approach towards screening.47-50 Benchmarking of individual practices may help in recognising high-risk individuals and those in need for treatment intensification.51,52 Studies on the long-term effect of specific interventions such as those in Sweden, in which primary care physicians are supported with lectures on BP treatment, a computerised decision support system with treatment recommendations, and yearly feedback on hypertension control, are ongoing.53 Other approaches involve the specific role of the general practice nurse to identify, recall and manage patients with uncontrolled hypertension.54
CONCLUSION
In summary, obese individuals of both sexes have a higher BP and LDL-C compared with overweight and normal weight individuals, and especially obese men younger than 50 years have elevated BP levels. Use of BP-lowering drugs did not revert BP back to levels normal for the specific age group, whereas cholesterol-lowering statins abolished the age-related increase in LDL-C. These data suggest that more attention is needed for active screening and treatment of cardiovascular risk factors.
ACKNOWLEDGEMENTS
The authors wish to acknowledge all participants of the Lifelines Cohort Study and everybody involved in the set-up and implementation of the study.
DISCLOSURES
The authors state that there are no conflicts of interest.
Grant support: Lifelines has been funded by a number of public sources, notably the Dutch Government, The Netherlands Organization of Scientific Research NWO [grant 175.010.2007.006], the Northern Netherlands Collaboration of Provinces (SNN), the European fund for regional development, Dutch Ministry of Economic Affairs, Pieken in de Delta, Provinces of Groningen and Drenthe, the Target project, BBMRI-NL, the University of Groningen, and the University Medical Center Groningen, the Netherlands. This work was supported by the National Consortium for Healthy Ageing, and funds from the European Union’s Seventh Framework program (FP7/2007-2013) through the BioSHaRE-EU (Biobank Standardisation and Harmonisation for Research Excellence in the European Union) project, grant agreement 261433. Lifelines (BRIF4568) is engaged in a Bioresource research impact factor (BRIF) policy pilot study, details of which can be found at: https://www. bioshare.eu/content/bioresource-impact-factor
REFERENCES