KEYWORDS
Older patients, frailty, qualitative research, caregiver experience, acute care, emergency department, quality of care
INTRODUCTION
Older patients represent an increasing proportion of emergency department (ED) admissions.1 Of the 90 EDs in the Netherlands, 75% report a structural increase in the admission of older patients.2
The increase in hospital admissions of older patients is a complex and challenging issue.3 Originally the EDs were designed and organised to treat and care for patients with a single acute illness. However, a large proportion of older patients suffer from multiple chronic diseases.1,4-6 In addition, the early identification of frail older patients as part of standard of care appears to be difficult in an emergency setting due to the hectic work environment,7 while this is thought to be essential to optimise the care provision for these patients.7-10
Frailty can be defined as the inability to withstand illness (or a stressor event) without loss of function or a loss of functional homeostasis.11,12 It is a dynamic state affecting an individual who experiences losses in one or more domains of human functioning (physical, psychological, social).13 Older patients who are frail do not cope well with change and disruptions,14 thereby increasing their risk of developing adverse events, dependence, morbidity, relapse, entry into a nursing home, or death.1,4,15,16 As a reaction to this, frailty instruments such as the Clinical Frailty Scale (CFS) and the Identification of Seniors at Risk (ISAR) score have been developed to determine existing geriatric vulnerabilities, such as functional and cognitive impairment.16 However, neither of these tools seem suitable to identify high-risk patients in an acute setting.17,18
Another issue while treating older patients is that they often receive care from multiple healthcare professionals from inside and outside the hospital, leading to a fragmentation of care and inefficiency in the acute care chain between the general practitioner, homecare, ambulance services, and the EDs and Acute Medical Units (AMUs) in the hospital. This increases suboptimal communication, the chance of errors, and delay in diagnosis and treatment.10 In contrast to elective care, there is also a scarcity of interventions (i.e. organisational, patient and next of kin-orientated, and professionalorientated interventions) which are developed and feasible for use in acute care.19 The reasons for this seem to be the focus on acute care, time pressures, and lack of resources.1 Hence, it seems there is no unambiguous answer on how to improve the acute care of older patients. The aim of this study is to start by involving the perspectives of healthcare professionals and other experts working in the acute care chain to gain more insight into the barriers and potential improvement opportunities of the different aspects of acute care. The main focus of the study will be on healthcare professionals working in secondary care who are involved in the triage process, the care process, and the discharge process of older patients.20 These insights may add to the knowledge needed to optimise or develop interventions that can help frail older patients with the transition of care and provide simple and time-saving tools which can support caregivers on the work floor.21
METHODS
Research setting and design
Twenty-two semi-structured interviews were conducted between March 2016 and May 2016 with healthcare professionals working in the acute care chain. We also included individuals who are experts on the topic of frailty and ageing in order to obtain a better understanding of current research and activities that are already being conducted to improve the acute care of older patients. Since the main focus was on secondary care, the majority of the interviews were conducted at the EDs of two hospitals in Amsterdam: an urban academic hospital with a level 1 trauma centre and a tertiary teaching hospital. However, as many older patients are referred to the ED by their general practitioner or arrive at the ED by ambulance also these primary healthcare professionals were invited to participate. In addition, a representative of a large community home care organisation in Amsterdam was approached for participation to gain more information on the discharge process from the hospital to home.
The academic hospital has a capacity of 733 beds, with approximately 55,000 hospital admissions each year and 31,000 ED visits a year. The tertiary teaching hospital has a capacity of 921 beds, with approximately 46,000 hospital admissions each year, and approximately 75,000 ED visits a year. The acute care of the academic hospital includes the ED and the acute medical unit. 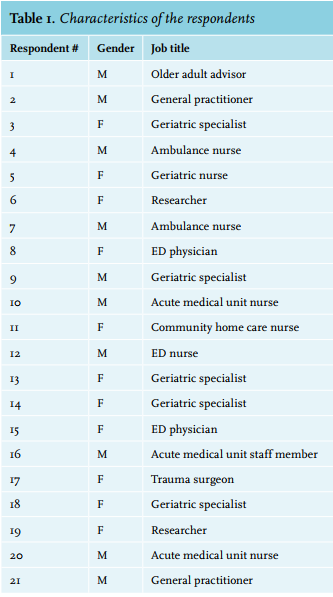
Participant selection
A brainstorm session was used to compose an inventory list of healthcare professionals and experts who would be eligible for participation. The different healthcare professionals and experts were contacted by mail or telephone to explain the goal of the project and to invite them to participate in the interview. All healthcare professionals and experts who were contacted agreed to take part in the study. Eighteen respondents were healthcare professionals working in primary (2 general practitioners, 1 community nurse) or secondary care (1 ED nurse, 2 ED physicians, 1 trauma surgeon, 5 geriatric physicians, 1 geriatric nurse, 2 ambulance nurses, 2 AMU nurses, 1 AMU physician). Three other respondents were experts working in the field of ageing, gerontology and geriatrics (2 researchers), one of whom participated in the organisation of activities and services dedicated to the Senior Friendly Hospital program (older adult advisor). Of the 21 respondents, two respondents were working in the tertiary teaching hospital. Upon agreement to participate, the researcher scheduled the date and location for the interview. The aim was to enrol enough healthcare professionals from secondary care to achieve data saturation.22 Data saturation was not achieved for the experts and the primary care providers due to the low number of respondents. The gender, job title and workplace of the respondents can be found in table 1.
Data collection
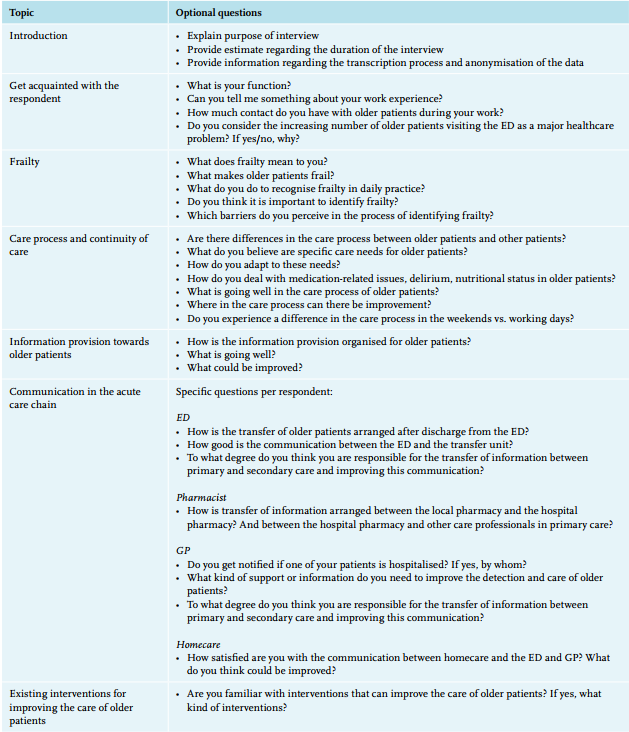
To gain insight into the experience of the respondents concerning the care of frail older patients a topic list was constructed for the interviews using recent literature regarding challenges in the delivery of acute care to older patients and interventions to improve the care of older patients (see Appendix). In addition, respondents were asked if they had any suggestions for improvement in the care of frail older patients. All the questions were open ended to enable the respondents to express their experiences and perspectives freely and in their own words. The interviews lasted 20 to 60 minutes (mean = 37 minutes). After obtaining the respondent’s consent, the interviews were audio-recorded and transcribed verbatim with support of the software program MAXQDA® 12 (VERBI software GmBH, Germany).
Data analysis
A thematic analysis was conducted in order to systematically pinpoint, examine, and record patterns (or ‘themes’) within the data. Thematic analysis is performed through the process of coding in six phases to create established, meaningful patterns. These phases are: familiarisation with data, generating initial codes, searching for themes among codes, reviewing themes, defining and naming themes, and producing the final report.23 To increase the reliability of the coding process, triangulation was used. Two researchers read, reread and coded two interviews individually (double-check) (DH and CB). The defining and naming of the codes were discussed by the researchers and an advisor from the acute care network, after conducting the first five interviews and after conducting all the interviews, until consensus was achieved (DH, CB, TW and HM). Eventually all codes were clustered together into main themes.
RESULTS
The following main themes were identified based on the data: 1) The concept of frailty, awareness concerning frail older patients, and identification of frailty, 2) Barriers in the care process of older patients within the acute care chain, 3) Optimising the discharge process of older patients, and 4) Improvement opportunities suggested by the respondents. The themes are illustrated by quotes that were translated into English.
Concept of frailty, awareness concerning frail older patients and identification of frailty
All respondents were positive about the fact that there has lately been an increased focus and awareness on improving the care of frail older patients. This focus, in their opinion, had been insufficient in the past.
‘Yes it is very positive, but I think the level of awareness is still too low. I notice that we struggle to improve this issue [….]. We know it is a must, but the older patient is still bogged down in daily practice.’ (R17, Trauma surgeon)
A large number of respondents stated that the identification of frailty is a major problem in the care of older patients. However, there was no consensus between respondents on the best way of identifying frailty. Some recommended the use of screening tools which are provided by the national improvement program for hospitals, or physical strength tests. Other respondents mentioned that in everyday practice they solely use their clinical acuity and intuition.
‘You use a different way of observing older patients. You look at the ‘normal’ patient history but you should also use a broader perspective. So you really need more tools to identify older frail people. It is less straightforward compared with the care of younger patients.’ (R13 Head of Geriatric Unit, Geriatric specialist, Academic Hospital)
Additionally, respondents mentioned different aspects of the term ‘frailty’. The four domains represented in the literature – physical, mental, social and cognition – were mentioned independently of each other. Respondents indicated that frailty was a difficult concept to explain due to the fact that the different aspects of frailty are interconnected. A few respondents mentioned all four domains. The domain ‘physical’ was mentioned by most respondents as an important aspect of frailty, in particular problems concerning comorbidity, but also aspects such as the risk of falling, level of mobility and the ability to take part in a conversation were mentioned.
The second main aspect of frailty commented on by many respondents is the social aspect. The living situation of older people: whether they live alone and whether they have a strong social network has a strong effect on frailty. Besides the social network, also the socioeconomic status is mentioned by respondents, whereby a higher socioeconomic status has a direct influence on the capability to organise care. Cognition was mentioned by a few respondents, while cognition is known to be associated with medication compliance and self-management.24 The mental aspect of frailty was also mentioned by some of the respondents as a factor that influences frailty. These respondents described the mental aspect of frailty as the perceived willpower and drive to live.
‘Yes, it is always very difficult, because frailty is a very broad concept. I think an older person is frail when there are deficiencies on multiple domains: physical, mental, social, functional. And even if you are so physically ill, you may not be frail when you are functioning well in the other domains. Frail people often have problems on multiple domains.’ (R13, Head of Geriatric Unit, Geriatric specialist, Academic Hospital)
Barriers in the care process of older patients within the acute care chain
Most respondents mentioned that they experienced differences in the care process between older patients and other patients. This difference was due to an increased focus on polypharmacy, drug rehabilitation, and challenges related to communication when treating older patients.
Communication barriers: ‘There are doctors who talk too fast, talk too loud, have a poor articulation, and who use difficult words. Well those are a few factors that are not really adapted to older patients.’ (R1, Advisor for older patients)
Communication barriers: ‘When I look at the interns and residents I get shivers down my spine. Once they recognise frailty, they set a tone of ‘well sir…’. A person may be delirious or may not understand everything, but they do not like the patronising way physicians speak. […] If someone has dementia, I still think the communication should be in a mature manner. There is a lot to gain by involving older people in the right way.’ (R9, Geriatric specialist)
Communication barriers: ‘Yes, I notice that older people want paternalism, where the doctor makes all the decisions. Young people are often more critical concerning their care. For older people this could be a pitfall, because older people are afraid to speak out if they have doubts about something…. (R19, Researcher)
The bottlenecks mentioned were mostly capacity problems of the acute care chain, staff limitations and capacity, challenges related to the continuity of care, a lack of facilities suited to older patients, and the lack of a generalist approach. Due to staff limitations, it is not always possible to ask a geriatric specialist for a consult at the ED, which is sometimes preferred when there is a suspicion of malnutrition, delirium or an increased fall risk. A few respondents also commented that there are differences in the quality of care throughout the week due to the limited availability of experienced professionals during non-office hours. Four respondents mentioned the lack of facilities for older patients with impaired mobility or cognitive capacity. These patients could benefit from adjusted toilets, private examining rooms and special patient leaflets. The lack of a generalist approach results in an accumulation of consultations by different specialists which can lead to incorrect or incomplete information in the patient record, for example about the choice of treatment or whether to treat or not.
Capacity problems: ‘The number of patients arriving at the ED is sometimes so large that we reach our maximum capacity. And sometimes we must refuse an older patient, which means that the older patient must go to another hospital. Well that can also be a risk, the other hospital is not quite familiar with the patient. The transfer to the other hospital, in itself, may also not always be beneficial for the patient. The whole region struggles with this, certainly in the winter months.’ (R8, ED staff member, Academic Hospital)
Continuity of care: ‘….Most patients arrive at the ED during office hours, but for those patients arriving in the evening or in the weekend it is very difficult to arrange aftercare. I think the contact with the primary caregivers in the weekend and evening is completely disconnected. Or the contact is very one sided. […].’ (R17, Trauma surgeon)
The need for information and tools for treating older patients: ‘Especially when we realise that 25% of the ambulance rides concerns geriatric patients, it would be useful to have a protocol or, at least, alarm signals, key features, small interventions, what are you supposed to do or not to do.’ (R15, Medical manager ambulance, ED specialist, Peripheral Hospital)
Only two respondents, the advisor of older patients in the academic hospital and the geriatric specialist, mentioned the social aspect as a very important aspect in the care process. The advisor of older patients also mentioned the attention of care providers for the human element in the care process.
‘If you are an older person, then who is caring for the plants? That is very important for an older patient,… or who takes care of the dog or cat. If there is interest for these things, then the human aspect is emphasised. The human aspect, such as family, animals, plants, is important to consider in the care process. Not only if you have taken your medication.’ (R1, Advisor for older patients, Academic Hospital)
Optimising the discharge process for older patients
The respondents mentioned several elements they considered important in the discharge process of older patients. Two respondents commented that involving a transfer nurse in the discharge process was imperative for a smooth transition from hospital back home or to a nursing home. The majority of respondents also mentioned the importance of obtaining an overview of the home situation of the older patient before discharge. A few respondents emphasised the importance of a standardised discharge process since, in the current situation, there is often too little time for an extensive discharge conversation and the discharge letter is often delayed or incomplete, especially with respect to contextual and personal information.
‘Especially the communication, the anticipation, the available time for discharge and how to discharge, these parts should be improved.’ (R16, Medical manager AMU, internist, Academic Hospital)
Many respondents mentioned a lack of agreement between the primary and secondary care providers concerning the responsibility for initiating contact. Arranging the transfer of patients is also experienced as a laborious undertaking, for example because the accessibility of rehabilitation centres is problematic and because of the complex paper-based process. As a result, patients often have to stay longer in the hospital than desired while they are not in need of medical treatment.
‘The AMU is also an “extension tube”. This entails that there are people in the hospital who could be discharged but for whom there is no room available in a rehabilitation centre and nursing home. That I think is also a concern.’ (R10, Nursing head of AMU, nurse, Academic Hospital).
‘Well I have to say honestly, when an older patient has to be admitted to the hospital, I am also not the first to contact the secondary care providers to say that I changed the medication yesterday. Let me be honest, I can improve on this. Although I think secondary care has to improve more than we do. This is due to the role distribution. The general practitioner should get the central role, but that only works if everyone is reporting back. (R21, General practitioner)
Improvement opportunities suggested by the respondents
During the interviews several interventions were mentioned which could potentially improve the care of older patients. In order to achieve a more holistic approach and thereby improve the care of older patients, respondents argued that regular consultations with geriatric specialists could be beneficial. Also the stimulation of interdisciplinary teamwork between departments which have a high number of frail older patients such as neurology, internal medicine, traumatology, orthopaedics and the AMU was mentioned as a possibility to increase the efficiency and quality of care. The ambulance personnel mentioned the implementation of a special protocol for older patients who are transported by ambulance. While there are special protocols for children there is no protocol or guideline for older patients. The respondents also argued that it would be helpful if older patients were to carry some kind of ‘medical passport’ in which essential information about their health is documented, such as medication, allergies, hearing, walking and visual aids, and advance directives).
To improve the communication and information between primary and secondary care, respondents mentioned that, especially during the weekends, the preferred contact options (phone/fax) between the ED, the general practitioner and home care about follow-up care should be more transparent and easily available. Another respondent suggested the use of the SBAR (Situation, Background, Assessment and Recommendations) technique25 to streamline information and improve the communication and collaboration between care providers in primary and secondary care. The discharge letter also plays an important role in the information exchange between care providers. Currently, respondents argue that the discharge letter is often incomplete or sent out too late which can lead to delay in follow-up.
Finally, in relation to the communication between older patients and care providers, a few of the respondents suggested that a consult by phone with the patient after discharge could be an effective way to provide aftercare while simultaneously creating the opportunity to check whether the patient has understood all the information given during discharge (i.e. follow-up appointments, medication changes, changes in home care, provide contact details in case of questions after discharge, and points of attention when arriving at home).
DISCUSSION
An important conclusion emerging from this study is that despite the many challenges faced by the different healthcare professionals when treating older patients there is a lot of common ground which offers the opportunity to work together on improving acute care for frail older patients. Based on the interviews, four aspects could be identified within the themes which are critical for improving the acute care of older patients in the hospital, namely: early identification of frailty, optimising the continuity of care, structured information exchange between care providers in the acute care chain, and a more generalist and holistic approach. Since this study has an explorative design the improvements suggested are not evidence-based but based on the opinion of the healthcare professionals and experts. Despite this fact we would like to compare our findings with the existing literature.
There is general consensus that the currently used models of emergency care units (disease-oriented instead of patient-oriented) do not adequately respond to the complex and changing care needs of older patients.26,27 The lack of a generalist and holistic approach in the acute care chain is in concordance with the literature and can lead to a significant delay in the process of decision making, resulting in a prolonged ED stay and undertriage, especially in vulnerable and older (> 65 years) patients.28,29 The Royal College of Physicians recommended that hospitals will need more generalists and fewer specialists in acute inpatient care in order to deal with patients with multiple chronic diseases.30 This will create a team of clinicians who will promote timely, holistic and integrated hospital care. Especially the holistic aspect of care was considered to be important by the geriatric physicians and older adult advisor. They argued that in acute care, the human element of care is often missing, while this is very important for older patients who are often anxious and have difficulty understanding all the information. Hence, there seems a lot to gain by optimising the communication and care towards older patients, as healthcare professionals tend to be too paternalistic or patronising when caring for older patients.
To improve the information exchange there is a need for more uniformity and structure. The SBAR technique, which was also suggested by one of the respondents, has proven to be beneficial in improving the standardisation of communication in several studies conducted in hospitals and rehabilitation centres.25,31-33 Respondents reported that they need a truly collaborative team environment to improve the information transfer, but also training to obtain the right skills. This finding is in line with other studies that underline the importance of teamwork and communication in providing safe care.34,35 This has resulted in an increase in the use of, for example, crew resource management training to train healthcare professionals in non-technical skills,36 but also in the introduction of ‘transition coaches’ who can help streamline the information exchange between primary and secondary care.37,38
Regarding the identification of frailty, many of the healthcare professionals mentioned the need for interventions which increase awareness and knowledge regarding the identification of frail older patients. Evidence confirms that increased knowledge and awareness by healthcare professionals is a prerequisite to achieve a change in a working routine, such as making the identification of frailty a routine care step at the ED.34,39-41 In some cases it seems a geriatric specialists can help in improving the knowledge of the ED staff concerning the identification of frailty. Also, developing easy-to-use standardised geriatric assessments tools, such as the frailty index, questionnaires or indicators, for the identification of frailty in an acute care setting could potentially be beneficial.21 A recent study showed that directly available clinical data describing disease severity and geriatric vulnerability can be used for prediction in hospitalised older patients,42 and that a combined outcome measure can successfully predict 90-day composite outcome and 90-day mortality in older emergency patients.42 In addition, the use of broad multidisciplinary teams to assess, organise and coordinate the care of older patient groups (referred to as comprehensive geriatric assessment) are being used for the identification of frailty in hospital EDs worldwide.10
Strengths and limitations
Some strengths and limitations need to be addressed. First, a strength of this study is that we included many different healthcare professionals and experts working in acute care. Secondly, the qualitative approach of this study offers a perspective of the respondents’ behaviour, needs, and desires. This study also has some limitations. First, the diversity and full scope of the acute care chain might not be perfectly reflected, since only three respondents were working in primary care, and the respondents working in secondary care were almost all from the same hospital. In the Netherlands there is a considerable difference in the hospital population of an academic hospital and peripheral hospital. Peripheral hospitals in rural settings often have more direct communication with primary care organisations, which makes it easier to communicate and organise appropriate care for older patients.43 Secondly, translation of the quotes from Dutch to English may have affected the context and meaning of the quotes. Hence, this exploratory study with in-depth interviews on the acute care chain for frail older patients should be replicated in other districts in the Netherlands to see if there are differences in findings.
CONCLUSION
Early identification of frailty, improving continuity of care by means of structured information exchange between care providers, and a more generalist care approach were identified as the most important improvement opportunities in the acute care of older patients. More collaboration seems to be needed in the future in order to share experiences, expertise and develop potential improvement strategies for the acute care of older patients.
ACKNOWLEDGEMENTS
We thank the care providers who were interviewed for their time and for sharing their experiences.
DISCLOSURES
All respondents provided consent to participate prior to the start of the interview. Ethics approval by an ethics committee was not applicable.
The authors declare that they have no competing interests and no financial support was received.
All data are available from authors upon request.
REFERENCES
APPENDIX
Topic list