KEYWORDS
Acute retroviral syndrome, functional cure, HIV reservoir, HIV transmission, post-treatment control, primary HIV
INTRODUCTION
Human immunodeficiency virus-1 (HIV) acquisition often elicits a severe inflammatory response and leads to irreparable damage to the immune system. The initial phase that follows HIV infection is known as primary HIV infection (PHI) and can be defined as the interval from the detection of the virus (HIV-RNA) in the plasma until the establishment of a stable plasma HIV-RNA level (viral set point) in the presence of evolving anti-HIV antibody reactivity.1 Initiating antiretroviral therapy (ART) during the acute phase of HIV infection reduces the inflammatory response, lowers the viral set point2,3 and can lead to a more rapid and robust immunological recovery compared with a later start. Early in the infection, a viral reservoir of memory CD4+ T cells with viral DNA integrated into the host DNA is formed. Viral transcription in these cells is nearly absent, which hinders immunological recognition and elimination. Starting ART immediately during the early phase of infection can reduce the size of this reservoir.4-6 Moreover, since patients are most contagious during PHI due to high viraemia,7,8 prompt treatment initiation reduces viraemia and thereby interrupts onward transmission. For these reasons, immediate initiation of treatment upon a positive HIV test is now recommended by the current international guidelines.1 Unfortunately, PHI remains a diagnosis that is frequently missed and patients are often unaware of having PHI at a time when they are particularly infectious. Awareness among at-risk patients as well as clinicians of the possibility of PHI is therefore of vital importance. Here we describe the pathogenesis, clinical presentation, and impact of treatment of PHI on individual and public health.
PATHOGENESIS OF PHI
To this day, the viral reservoir remains one of the major barriers to curing HIV. After entering the body, HIV reaches the draining lymph nodes where it rapidly replicates in CD4+ T cells and subsequently spreads throughout the body.9 Already during this phase, HIV integrates in the genome of long-lived CD4+ T cells forming a stable latently infected reservoir.10 CD4+ T cells in the gut-associated lymphoid tissue are particularly affected and their rapid depletion results in chronic damage to the gut mucosa.10,11 HIV replicates in the lymphoid tissues and plasma viraemia increases exponentially while the adaptive immune system is still mounting a response. This ramp-up viraemia coincides with a large burst of pro-inflammatory cytokines produced by innate immune cells, including natural killer (NK) cells. NK cells help control viral replication through recognition of infected cells via specific types of receptors.12 Although generally the NK cell response against HIV is insufficient, marked differences in anti-HIV effects can be appreciated based on their maturation status.13 The NK cell compartment in any individual consists of more or less matured populations, resulting in a unique profile. A more mature NK profile improves several virological and immunological markers in patients with PHI. These patients have lower viral load set points and show a better early virological response to ART initiated during PHI.14 During the adaptive immune response, B cells produce antibodies and CD8+ T cells mount a HIV-specific cytotoxic T cell (CTL) response. CD4+ helper T cells regulate the CTL response, but are also infected by HIV. As a consequence, they are killed by CTL or prone to virus-induced pyroptosis.15 These combined effects result in a steep initial drop in CD4+ T cells during the first stages of PHI. This is only partly reversed through limited control over viraemia in later stages. Despite its magnitude, the immune response during PHI is unable to clear these reservoir cells. Interventions during PHI before a long-lived reservoir is established present an opportunity to achieve sustained control over the virus, and may even lead to a cure.
CLASSIFICATION OF THE STAGES OF PHI
Figure 1 provides an overview of the consecutive clinical stages following initial HIV transmission. The stages as classified by Fiebig are defined by a stepwise detectability of HIV antigens and HIV-specific antibodies using different diagnostic assays.10,16 Successful HIV transmission marks the start of the eclipse phase. During this phase, the infection is established but viral markers in the blood are not yet detectable by routine diagnostics. At the end of the eclipse phase, the emergence of plasma HIV-RNA above the level of detection (approximately 11 days post infection) marks the start of Fiebig stage I. The detection of p24 antigen one week later marks Fiebig stage II. The plasma HIV-RNA increases exponentially and peaks between day 21 and 28 post infection, after which a slower decrease in plasma viral RNA follows. Fiebig stages III to V are based on the sequential detection of HIV-specific antibodies by enzyme-linked immunosorbent assay (ELISA) or Western blot. Progression to Fiebig VI marks the onset of the early chronic stage during which the plasma HIV-RNA stabilises and a viral set point is established. 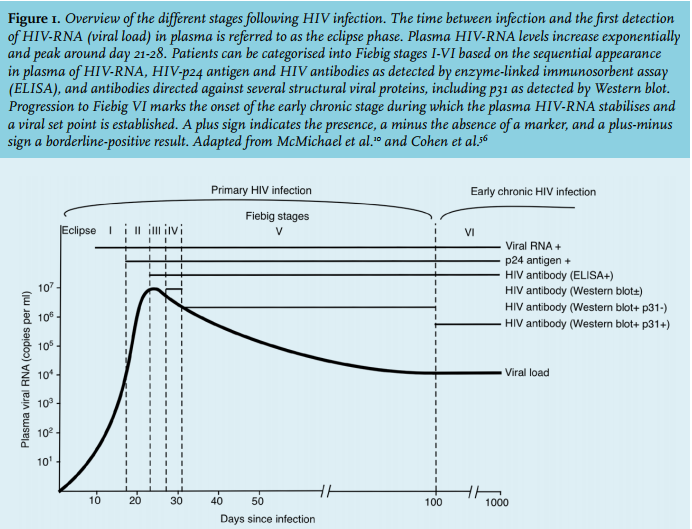
CLINICAL PRESENTATION
Around two weeks after HIV acquisition, patients commonly experience symptoms that suggest a mononucleosis-like illness known as acute retroviral syndrome.17-21 The acute illness may last from a few days to more than 10 weeks, but generally the duration is less than 14 days.22,23 The estimated proportion of patients who seek professional medical care for their PHI-associated symptoms ranges from 53% to 87%.17,20,24,25 One study estimated the prevalence of PHI among patients seeking care for fever or rash to be 0.5-0.7%.26 Unfortunately, when patients present at healthcare facilities, PHI is hard to recognise due to the brevity of the symptomatic phase and nonspecific symptoms. In addition, in spite of current guidelines recommending pro-active testing,27 the frequency of routine HIV testing of high-risk individuals by both primary and secondary care clinicians is low.28-30 In Kenya, Sanders and colleagues identified seven characteristics that are independent risk factors of PHI: a younger age (18-29 years), fever, fatigue, body pains, diarrhoea, sore throat, and genital ulcer disease.31 Based on those findings, they proposed and tested a targeted risk score algorithm to detect PHI.31,32 In the Netherlands, a similar PHI testing strategy was developed as part of the H-team, an initiative originally launched by the late Professor Joep Lange.33 This strategy includes a risk score algorithm aimed at men who have sex with men and involves standard of care HIV testing as well as a novel point of care (POC) RNA rapid test at the Amsterdam Public Health Service. Of 206 eligible men who presented for testing between August 2015 and January 2017, 17 men were newly diagnosed with HIV, 2 of whom were diagnosed as Fiebig I (RNA POC positive, p24 negative, antibody negative), 8 as Fiebig II (RNA POC positive, p24 positive, antibody negative), and 7 as Fiebig III-V (RNA POC positive, p24 positive and antibody positive).34 Although these findings show that effective screening strategies can lead to diagnosis of patients in the early Fiebig stages, various studies in both resource-rich and low-resource settings indicate that regardless of clinical criteria, identification of PHI remains difficult.19,21,22Table 1 presents a list of commonly considered differential diagnoses mimicking PHI in potential risk groups, including diagnostic tests that can help to differentiate. Given the wide range of symptoms associated with PHI, clinicians should have a low threshold to consider HIV testing. Moreover, awareness among clinicians of PHI in high-risk groups such as men who have sex with men, heterosexual individuals with multiple sexual partners, and migrants from areas with a high HIV prevalence is critical. When such high-risk patients present with signs and symptoms of syphilis, other STDs, or mononucleosis-like symptoms, clinicians must consider PHI as a possible co-infection or even the main cause of the clinical presentation. Finally, when known high-risk patients present with new symptoms associated with PHI clinicians should repeat HIV testing even if a very recent negative HIV test is available, because the diagnostic window of PHI is so narrow.35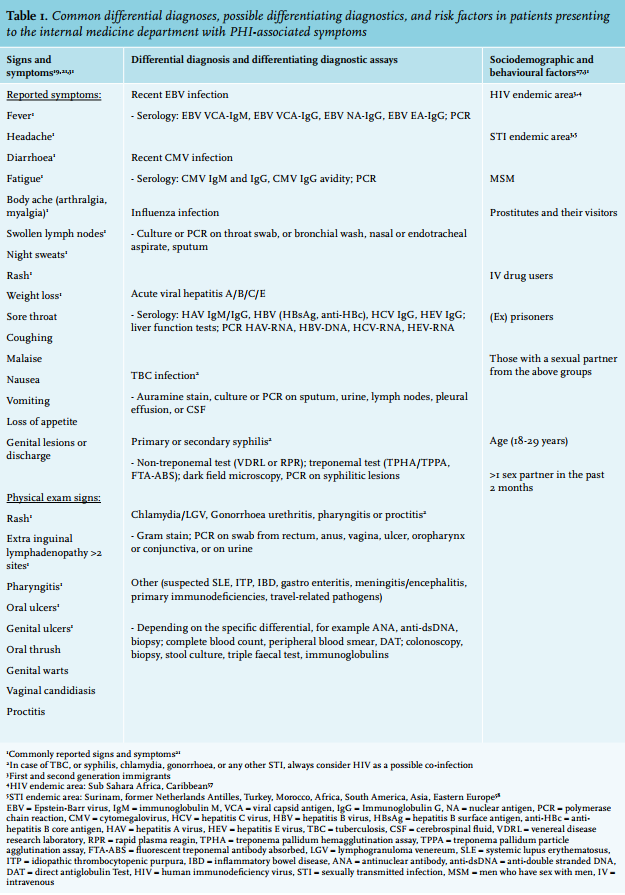
IMPACT ON PUBLIC HEALTH
In 2011, Cohen and colleagues highlighted the potential impact of treatment of HIV on public health by showing that initiating ART immediately after diagnosis almost eliminated the risk of HIV transmission to an uninfected person in heterosexual serodiscordant couples.36 Since PHI accounts for approximately half of onward HIV transmission in resource-rich settings,37 treatment of PHI presents an effective tool to prevent onward transmission. Indeed, modelling studies indicate that early detection of PHI and an immediate start of ART provide an important opportunity for prevention of transmission, potentially even for HIV elimination.38-40 Obviously, early ART initiation should not preclude patient support and risk reduction counselling, or other modifications of sexual risk behaviours.41 In the Netherlands, general practitioners, community health services and STI clinics diagnose the majority of HIV infections (approximately 60%).42 Unfortunately, observational studies found that PHI represents only 3.4% of all new HIV diagnoses.43 Even in low prevalence areas where repeated HIV testing will predominantly yield negative test results, identification of only a few additional cases of PHI due to increased screening and pro-active testing of high-risk populations is modelled to be cost-effective.44,45 Failure to identify PHI may compromise HIV prevention efforts and hinder the potential population-wide benefits. Therefore, continuous pro-active HIV testing of high-risk patients by healthcare professionals from all disciplines, and expanding coverage by including strategies such as HIV self-testing, are needed.46
IMPACT ON INDIVIDUAL HEALTH
The best practice for clinical management of PHI is a subject of ongoing research. Ananworanich and colleagues found that T cell depletion and HIV reservoir seeding begins in the earliest days after HIV infection, and that commencing ART during this crucial period limits CD4+ T cell destruction and the HIV reservoir size.47 These findings suggest a promising scenario where intervention with ART during PHI leads to favourable long-term viral and immunological outcomes compared with a deferred start of therapy. In recent years, three prospective, randomised controlled multicentre studies have shown individual health benefits of ART initiated during PHI.2,3,48 The Short Pulse Anti-Retroviral Therapy at Seroconversion (SPARTAC) trial is the largest multicentre randomised controlled trial to date involving 366 PHI patients.3 In this study, a 48-week course of ART during PHI resulted in significant CD4+ T cell improvement and a lower plasma viral set point after treatment interruption. The Dutch Primo-SHM trial involving 115 PHI patients showed a similar trend.2 The Setpoint study (ACTG-A5217) included 130 PHI patients and was in fact prematurely terminated due to better outcomes in the group receiving immediate treatment.48 Importantly, although these studies indicate that starting and then stopping treatment is a beneficial and potential therapeutic strategy, a large, long-term randomised controlled trial of patients with chronic HIV infection found treatment interruption to have harmful effects,49 and consequently current guidelines recommend uninterrupted treatment.1 Moreover, precisely which combination of antiretroviral medication presents the optimal treatment of PHI, and whether intensification of ART can yield greater benefits in reducing markers for HIV reservoir size and immune activation, is presently unclear. A small randomised controlled trial by Ananworanich et al. in which drugs that can block viral cellular entry (maraviroc), and integration (raltegravir) were added to a standard regimen with nucleoside reverse-transcriptase inhibitors (tenofovir and emtricitabine) and a non-nucleoside reverse-transcriptase inhibitor (efavirenz) did not show an additional effect in reducing the viral burden and HIV reservoir seeding in Thai individuals.50 Furthermore, while early intervention seems favourable, data on definite clinical endpoints such as mortality are still unavailable. Nonetheless, these findings support the rationale of ART initiation during PHI at the earliest stage possible, before the immune system suffers irreparable damage and the reservoir size is established.
POTENTIAL FOR CURE
Initiating ART during PHI offers the potential for what is known as a functional cure. A patient is considered functionally cured, or a post-treatment controller, when ART can be interrupted without subsequent rebound plasma viraemia or progressive loss of cellular immunity. The potential for achieving a functional cure when treatment is started during PHI is reflected by a number of studies. The case of the Mississippi infant is illustrative. Since the baby was born to an HIV-infected mother who had received no prenatal care, it began receiving full ART 30 hours after birth. ART was interrupted and the baby was withdrawn from care by the mother after 18 months of continuous ART, but surprisingly, this infant sustained an undetectable plasma viral load at the age of three years when re-entering medical care.51 Unfortunately, two months before reaching the age of 4 years viral rebound occurred and the girl had to be started on ART again. Similar observations were derived from the RV254/SEARCH 010 study, an ongoing prospective, longitudinal cohort of PHI patients in Thailand that was initiated in 2009. The authors of this study were the first to imply immediate treatment of PHI as a promising strategy to reduce reservoir formation to eventually achieve sustained drug-free viral remission.47 A landmark study on post-treatment controllers is the Viro-Immunological Sustained CONtrol after Treatment Interruption (VISCONTI) cohort.5 In this study, 14 post-treatment controllers were identified out of a much larger cohort of PHI patients who started ART during PHI and who subsequently interrupted ART after a median of three years. These 14 patients remained aviraemic for several years after ART interruption.5 The small viral reservoir and altered CD4+ T cell subsets in these individuals have been hypothesised to be contributing factors. In line with this assumption, post-treatment controllers are far less frequently observed when ART is started in the chronic stage of HIV infection. Other treatment interruption studies have identified similar patients.52 Furthermore, longer exposure to ART is associated with a greater chance of post-treatment control in patients with PHI,53 and previous evidence points towards uninterrupted treatment.49 Therefore, stopping ART in the context of a cure study should be carefully planned, HIV-RNA guided, and closely monitored. Unfortunately, clear markers to predict sustained virus control after treatment of PHI have yet to be elucidated. Clearly, post-treatment controllers hold an important clue with regard to future curative efforts, but for the majority of individuals including those with PHI, treatment interruption results in viral rebound and continuous ART remains a necessity.
CURRENT AND FUTURE PROSPECTS
In line with current guidelines, patients should be informed about the benefit of starting ART following PHI diagnosis, and be counselled about the high risk of transmission as long as they are highly viraemic, preventive measures, and the importance of notifying partners.1 The European AIDS Clinical Society (EACS) advises that clinicians should be familiar with local routes to ensure instant referral to an HIV specialised centre to start treatment as soon as possible, and preferably combine this with enrolment into clinical studies investigating HIV curative strategies.1 Such a study is the Netherlands Cohort Study on Acute HIV Infection (NOVA), part of the H-Team initiative, which intends to promote prompt linkage to care and immediate ART initiation in all PHI patients in the Netherlands. Such initiatives also offer opportunities for a detailed characterisation of the viral reservoir and could provide further insights into the early immune response to HIV. By obtaining a better understanding of the factors related to functional cure, such studies can help optimise treatment strategies and assist in identifying patients who could benefit most from future strategies to achieve post-treatment control, including cure strategies with therapeutic vaccination or specific agents targeting the HIV reservoir. While work on a future cure is in progress, other initiatives to halt onward HIV transmission are needed. For example, pre-exposure prophylaxis has been shown to be highly effective54,55 and thereby would present an important strategy to reduce the incidence of HIV infection and can aid in HIV elimination.
CONCLUSION
Greater clinical awareness of PHI among clinicians from all disciplines, pro-active and repeated HIV testing, and fast linkage to care in order to facilitate an immediate start of ART merit our attention. First, it helps to prevent onward transmission and could ultimately lead to HIV elimination. Second, it improves an individual patient’s health by limiting both reservoir size and immune damage. This could aid future efforts to achieve a functional cure. Ongoing studies involving patients with PHI remain a necessity, however. Thirty-five years on, more than 40 million people have died due to HIV globally. In the Netherlands, approximately 900 people still become infected with HIV every year. PHI remains a clinical and public health emergency that requires early diagnosis and immediate intervention. If we are to finally end the HIV epidemic, PHI should be on the agenda.
DISCLOSURES
All authors declare that they have no conflict of interest. No financial support was received for the conduct of this study or preparation of this manuscript.
REFERENCES