CASE REPORT
A 66-year-old male was admitted to the intensive care unit in respiratory distress. Medical history revealed type 2 diabetes mellitus, a small right-sided lacunary cerebral infarction and alcohol/nicotine abuse. Known prescribed medications were metformin, folic acid, clopidogrel, pravastatin, fosinopril, amlodipine, ranitidine and hydrochlorothiazide. Physical examination showed a very tachypnoeic patient using the accessory respiratory muscles, respiratory rate 40/minute, SatO2 85% with 15 litres/minute oxygen on a non-rebreather mask, blood pressure of 160/80 mmHg, heart rate of 100/minute and tympanic temperature of 37.3 °C. Blood gas analysis showed a metabolic compensated respiratory acidosis (pH 7.38, pCO2 7.0 kPa, HCO3- 30.6 mmol/l, base excess 4.4 mmol/l) and hypoxia (pO2 8.5 kPa, SatO2 90%). He was intubated and immediately mechanically ventilated. Laboratory results showed leucocytosis (35 x 109/l) and C-reactive protein of 39 mg/l. Chest X-ray (figure 1, panel A) showed extensive infiltration of the left upper lobe, suspicious for infectious pneumonia. We suspected a severe case of community-acquired pneumonia and started intravenous treatment with penicillin 6 million units a day and ciprofloxacin 400 mg three times a day.
In the next few days the patient did not improve. Urine testing on Legionella pneumophila and Streptococcus pneumoniae antigen was negative, as were blood/sputum cultures and PCR testing on bacterial and viral respiratory micro-organisms. CT scan (figure 1, panel B and C) showed dense consolidation with air bronchograms, suspicious for necrotising pneumonia. On day 3, a bronchoalveolar lavage (BAL) was performed, which showed no airway obstructions but large quantities of thin, bright, clear-white foamy sputum. Again, all cultures stayed negative. Eosinophilic pneumonia/pneumonitis was excluded by testing the BAL liquid on eosinophil count. His situation worsened and intermittent ventilation in a prone position was needed. Finally he was treated with high-dosed steroids for a ‘cryptogenic organising pneumonia’. Again there was no improvement.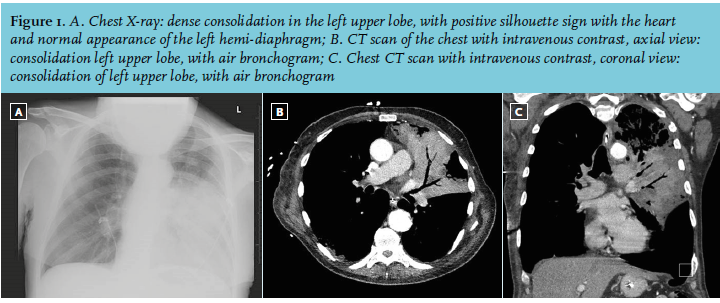
WHAT IS YOUR DIAGNOSIS?