KEYWORDS
Checkpoint inhibition, thyrotoxicosis, thyroiditis, lung cancer, immune related adverse reactions
INTRODUCTION
The immune checkpoint-blocking antibody nivolumab is a promising new drug to treat different malignancies. It promotes immune responses by blocking programmed death-1 (PD-1) receptor immune cells. Patients with lung cancer treated with nivolumab have a better overall survival, response rate, and progression-free survival than those treated with chemotherapy.1,2 One out of five patients show a durable tumour response, but a good biomarker is still lacking.3 Besides its benefits, nivolumab may cause immune-related adverse reactions such as skin toxicity (31%), gastrointestinal toxicity (11%), pneumonitis (3%), thyroid dysfunction (3%), and hypophysitis (< 1%).4 Thyroid dysfunction is expressed as hypothyroidism (7%), hyperthyroidism (1%), and thyroiditis (< 1%), mostly described around week 12 after the start of therapy with nivolumab.5-7 Thyroid dysfunction occurred more often in patients treated with anti-PD-1 than in patients treated with CTLA-4 immune checkpoint inhibitors such as ipilimumab (1.8-9%).8-10 Another PD-1 blocker, pembrolizumab, has also been related to thyroid dysfunction, such as hypothyroidism and hyperthyroidism, 10.1% and 6.5% respectively.11,12 Cytology in these patients on pembrolizumab shows lymphocytic thyroiditis with multinucleated giant cells.13 The optimal treatment and the underlying pathophysiological mechanism causing thyrotoxicosis as an immune-related adverse reaction during treatment with anti-PD-1 have not yet been established.14 We speculate that a transient destructive thyroiditis is the most likely underlying pathophysiology and, therefore, prescription of beta blockers to reduce symptoms is the most logical approach.
CASE REPORTS
We report two cases with temporary thyrotoxicosis turning into hypothyroidism during nivolumab treatment. Both patients had a clinical benefit from nivolumab treatment with a partial tumour response and are still on nivolumab treatment.
Case report 1
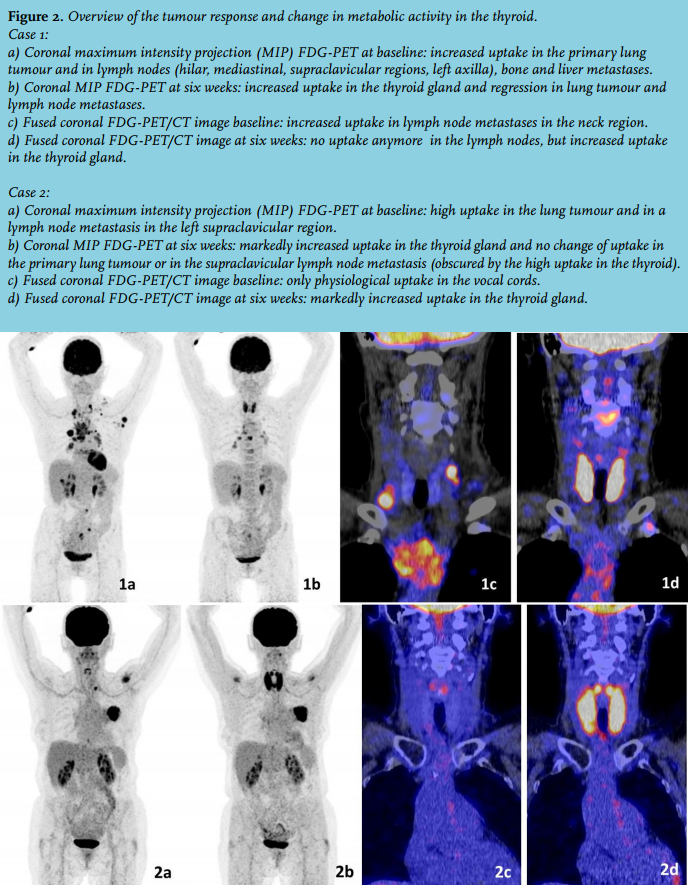
A 63-year-old female, diagnosed with squamous-cell non-small-cell lung carcinoma (NSCLC) stage cT3N3M1b developed symptomatic thyrotoxicosis: progressive fatigue, excessive sweating, weight loss, tachycardia, and a non-tender, enlarged, diffuse goitre, four weeks after initiation of treatment with nivolumab. Laboratory findings revealed FT4 47.5 pmol/l (11.0-19.5), FT3 10 pmol/l (4.4-6.7), thyroid-stimulating hormone (TSH) 0.020 mU/l (0.5-4.0), and negative thyroid antibodies (thyrotropin binding inhibiting immunoglobulins (TBII), anti-thyroid peroxidase (TPO)). Medical history was negative for thyroid disease. Second-degree relatives were known to have hyperthyroidism and goitre. In the assumption that a possible Graves’ disease had been induced by immunotherapy, temporary treatment with atenolol (50 mg daily) and methimazole (30 mg daily) was started, resulting in immediate resolution of the symptoms. Two weeks later the FT4 normalised (figure 1), the clinical symptoms improved, and TBII was found to be negative, leading to discontinuation of the methimazole. 18F-fluorodeoxyglucose positron emission tomography computed tomography (FDG-PET/CT) performed six weeks after starting nivolumab showed a partial tumour response, but also symmetrically increased uptake in the thyroid, which was not present at baseline FDG-PET/CT (figure 2). Levothyroxine was started eight weeks after starting nivolumab therapy when hypothyroidism occurred (FT4 7.2 pmol/l). Anti-TPO levels were < 33 IU/ml before therapy and 78 IU/ml four weeks after starting nivolumab (negative < 100 IU/ml). Moreover, Sjögren’s syndrome was diagnosed based on typical symptoms and elevated Sjögren syndrome antigen antibodies 3-4 months after initiation of the nivolumab therapy. 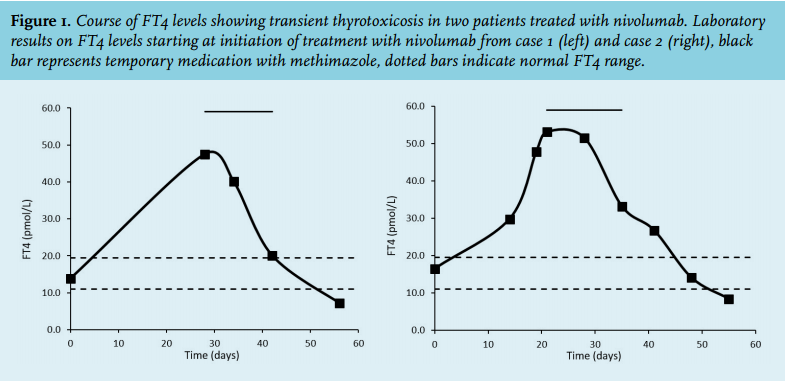
Case report 2
A 71-year-old female, diagnosed with squamous-cell NSCLC stage T2aN2-3M1b presented with symptoms of thyrotoxicosis: excessive sweating, palpitations and a diffuse enlarged and tender thyroid, two weeks after initiation of treatment with nivolumab. Laboratory findings revealed FT4 53.1 pmol/l, FT3 14.3 pmol/l, TSH 0.010 mU/l, and negative thyroid antibodies (TBII, anti-TPO). Medical and family histories were negative for thyroid diseases. Atenolol (50 mg daily) and methimazole (30 mg daily) were started because of the suspicion of Graves’ disease, especially based on subtle eye signs. Nivolumab was continued and treatment with methimazole was stopped after two weeks because of declining FT4 levels (figure 1) and the rising suspicion of a temporary phenomenon. Six weeks after starting nivolumab a FDG-PET/CT scan showed symmetrical, increased FDG uptake in the thyroid, which was not visible at the baseline FDG-PET/CT, without clear reduction in metabolic activity or size of the primary tumour in the lung, see figure 2. Eight weeks after the start of nivolumab therapy hypothyroidism developed (FT4 8.4 pmol/l) and levothyroxine was started. Anti-TPO levels were < 33 IU/ml after initiation of therapy and changed to 65 IU/ml over time.
A tracer dose of radioiodine was deemed not to be informative regarding the recent repeated gifts with iodinated contrast in both patients. Neither cytology nor histology from the thyroid was obtained.
CONCLUSION
Both cases demonstrate a transient thyrotoxicosis already within 2-4 weeks after starting treatment with nivolumab, with a rapid transition to hypothyroidism. Temporary treatment with a beta blocker may be sufficient. Afterwards thyroid hormone substitution may follow, whether or not in the long term. We speculate that the underlying pathophysiological mechanism is a transient destructive thyroiditis, a conclusion based on the relatively rapid resolution and temporarily increased FDG uptake.12 Therefore thionamides should not be used during the initial period with thyrotoxicosis, unless there are clear signs of Graves’ disease, or a more sustained thyrotoxicosis.
Since the number of patients treated with nivolumab is expected to increase, our cases should increase awareness of the evaluation and management of this form of thyrotoxicosis.
DISCLOSURES
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
REFERENCES