KEYWORDS
Direct oral anticoagulants, rivaroxaban, tubulointerstitial nephritis
INTRODUCTION
Acute tubulointerstitial nephritis accounts for approximately 10-15% of all cases of acute renal failure.1-3 More than two-thirds of these cases are drug-induced.4 The incidence of tubulointerstitial nephritis has increased due to the increasing number of prescribed drugs and easy availability of over-the-counter medication. Drugs commonly associated with tubulointerstitial nephritis are non-steroidal anti-inflammatory drugs (NSAIDs) and antibiotics, such as penicillins. However, many other drugs can induce tubulointerstitial nephritis as well. In this report, we describe a case of tubulointerstitial nephritis caused by a direct oral anticoagulant (DOAC), rivaroxaban. Rivaroxaban is prescribed for several indications, including the prevention of systemic embolic events in patients with non-valvular atrial fibrillation. Although rivaroxaban is prescribed frequently and has been registered since 2008, we are the first to report a case of rivaroxaban-associated tubulointerstitial nephritis.
CASE REPORT
An 82-year-old male presented to his general practitioner because of fatigue, weakness and weight loss for three weeks. The patient’s history revealed hypertension, a DDDR pacemaker for a third-degree atrioventricular block and decreased renal function of unknown cause (estimated glomerular filtration rate (eGFR) 39 ml/ min/1.73 m2 ). His daily medication comprised amlodipine 5 mg, enalapril 20 mg, hydrochlorothiazide 12.5 mg and omeprazole 40 mg. Three weeks before presentation he was diagnosed with atrial fibrillation and started on rivaroxaban 15 mg. Several days before presentation the patient had stopped taking rivaroxaban because of his symptoms. Other medication had not been changed and the patient was not taking any over-the-counter medication or supplements. Laboratory assessment revealed an eGFR of 9 ml/min/1.73 m2 and the patient was referred to the hospital. At physical examination the patient’s blood pressure was 148/81 mmHg, pulse rate 62 beats/min and temperature of 35.8 °C. The patient appeared euvolaemic and further physical examination was unremarkable. Results of laboratory analysis including urinalysis are provided in table 1. Renal ultrasound showed normal sized kidneys of 12.2 and 13.6 cm and no postrenal obstruction.
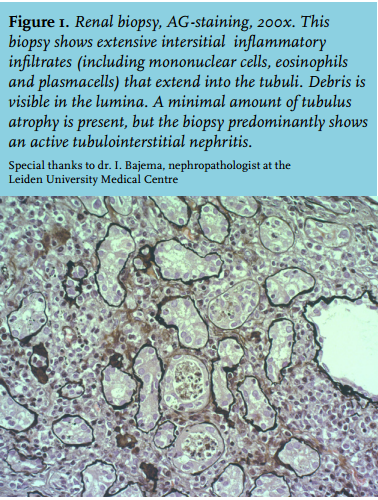
Resonium and sodium bicarbonate were started, as well as ciproxin 500 mg to treat a urinary tract infection until urinary cultures proved negative after five days. The patient was also started on dialysis because of refractory hyperkalaemia. Renal biopsy was performed and showed extensive tubulointerstitial nephritis, as depicted in figure 1. As renal function had declined after rivaroxaban had been started and no other drugs were altered, rivaroxaban was considered the most likely causative agent. The patient was started on 40 mg prednisone for two weeks followed by a taper schedule of 5 mg per week. The patient continued dialysis for six weeks until renal function improved sufficiently. Eight weeks after presentation to the hospital the eGFR had recovered to 34 ml/min/1.73 m2.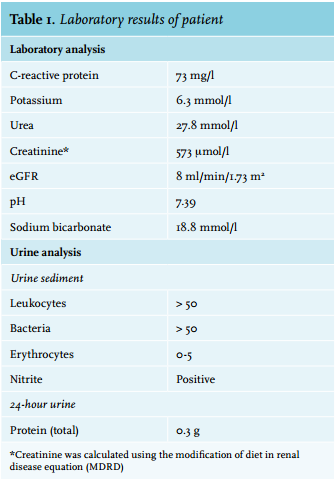
DISCUSSION
DOACs such as rivaroxaban are prescribed frequently because of advantages over vitamin K antagonists, including a quicker onset and offset of effect and eliminating the requirement for regularly monitoring coagulation.5,6 Recent publications have shown that rivaroxaban has a similar efficacy and safety to vitamin K antagonists in terms of risk and outcome of bleeding.7,8 However, less information exists about long-term safety and side effects. Unlike vitamin K antagonists, a commonly reported side effect (1-10%) of rivaroxaban is renal impairment. The pathophysiology remains unknown. This case report is the first to show rivaroxaban-associated tubulointerstitial nephritis. A literature search on DOAC-associated tubulointerstitial nephritis revealed one case of dabigatran toxicity associated with allergic interstitial nephritis, presented at a clinical meeting. However, no renal biopsy was performed to affirm the suspicion.9 Lareb, the Dutch centre for the registration of drug side effects, received two earlier reports of tubulointerstitial nephritis attributed to rivaroxaban.10 To date, the World Health Organisation (WHO) has reported 20 incidents of rivaroxaban-associated tubulointerstitial nephritis.11 It is unclear whether the cases reported by Lareb and WHO are biopsy proven.
The pathophysiology of drug-induced tubulointerstitial nephritis is most likely a secondary immune reaction. This hypothesis is supported by the lack of a dose-dependent relationship, coinciding presence of extrarenal manifestations of hypersensitivity in many cases, and recurrence after accidental re-exposure to the same or closely related agent.12 Risk factors for drug-induced tubulointerstitial nephritis include pre-existing chronic kidney disease, age, diabetes, hypoperfusion, and duration of therapy. In our case, it was an elderly patient with pre-existing impaired kidney function.
Clinical suspicion of drug-induced tubulointerstitial nephritis should arise when an unexplained increase in the serum creatinine level or an abnormal urinalysis is present, when fever, rash and/or eosinophilia occur and when malaise occurs shortly after starting a new medicine.13 Mild to moderate proteinuria is often present and sediment usually shows white blood cells, including white blood cell casts. The presence of eosinophilia has a low predictive value, and the absence does not exclude the possibility of drug-induced tubulointerstitial nephritis.14 A relatively normal urinalysis should not exclude the diagnosis. Renal biopsy is the only definitive method of establishing the diagnosis of tubulointerstitial nephritis. Irrefutable proof of the cause of tubulointerstitial nephritis is hard to acquire, however, in this case rivaroxaban seems the most likely causative agent. Reintroduction of rivaroxaban could confirm the causative relationship, but was considered unethical because of the severity of the disease.
Treatment of tubulointerstitial nephritis consists of discontinuation of the potential causative drug. The effectiveness of glucocorticoids remains unclear, as research shows inconsistent findings.13,15 In general, the outcome of drug-induced tubulointerstitial nephritis is good; upon cessation of the causative agent, (partial) recovery of renal function occurs in 85-90% after several weeks to months.2 In our patient, rivaroxaban had already been discontinued shortly before presentation and renal function had almost completely recovered to pre-existing level in eight weeks.
In conclusion, we present a case of biopsy-proven tubulointerstitial nephritis associated with rivaroxaban, which to our knowledge has not been described previously. As DOACs are increasingly being prescribed, this severe side effect might be encountered more often in the future.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES