KEYWORDS
ANCA-associated vasculitis, end-stage renal disease, renal screening practice
INTRODUCTION
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a life-threatening disease that affects multiple organ systems.1,2 By the time it is diagnosed, renal involvement is present in 60-80% of patients.3,4 Renal involvement in AAV progresses rapidly and may lead to the need for renal replacement therapy within days.5 In AAV patients with kidney damage it is generally recommended to immediately start aggressive immunosuppressive therapy (cyclophosphamide or rituximab in combination with glucocorticoids with or without plasma exchange) in order to prevent progression to end-stage renal disease (ESRD).6-8
Deterioration of renal function in AAV is often preceded by urinary abnormalities, such as erythrocyturia and/ or proteinuria.9-12 A recent study in AAV patients with crescentic glomerulonephritis showed that renal outcomes were similar between patients with and without renal impairment at diagnosis.11 This indicates that baseline renal function alone is a poor marker for renal outcomes in AAV. The benefit of aggressive immunosuppressive therapy in patients with crescentic glomerulonephritis and a preserved renal function has not been addressed in randomised controlled trials so far. Nevertheless, observational data showed better renal outcomes if these patients are treated with cyclophosphamide.11 It is therefore suggested to treat patients with renal AAV and a preserved renal function with aggressive immunosuppressive therapy, similar to patients with renal impairment at presentation.11,13
Early and complete screening for renal involvement is required in order to immediately start adequate treatment. Recent guidelines recommend screening for renal involvement early in the diagnostic process.14 So far, the implementation of renal screening and its effects on renal outcome in AAV have not been studied. The aim of the present study is to evaluate whether screening for renal involvement is timely and complete in clinical practice in a teaching hospital in the Netherlands and to determine whether the failure of adequate screening had an impact on renal function after 12 months and the development of ESRD. Furthermore we investigated the diagnostic properties of urine analysis that preceded renal biopsy-proven AAV.
MATERIALS AND METHODS
We performed a retrospective cohort study in the Northwest Clinics, a teaching hospital group in Alkmaar and Den Helder in the Netherlands. The local medical ethics committee approved the study and waived the requirement for informed consent. Patients who were positive for ANCA proteinase-3 (PR3) or myeloperoxidase (MPO) between February 2005 and February 2015 were screened for the clinical diagnosis of AAV, in accordance with Watts algorithm entry criteria for epidemiological studies.15 All AAV patients who were diagnosed within the Northwest Clinics were included in the study. ANCA serology was assessed by indirect immunofluorescence on neutrophil substrate (NOVA Lite® ANCA, INOVA Diagnostics Inc, San Diego, USA) and, if positive, followed by immunoassays for the detection of antibodies to PR3 and myeloperoxidase MPO (Autostat™ II Anti-PR-3 and Anti-MPO ELISAs, Hycor Biomedical Ltd, UK, from February 2005 until August 2012, and EliA™ PR3S and EliA™ MPOS run on a Phadia 250 analyser, Thermo Fisher Scientific, Immunodiagnostics, Sweden from August 2012 until the end of the study period).
Medical records of all enrolled AAV patients were reviewed for patient demographic data, the department diagnosing AAV and the date of diagnosis. Furthermore data on renal outcome, including serum creatinine, estimated glomerular filtration rate (eGFR), using the abbreviated Modification of Diet in Renal Disease (MDRD) equation16 and the development of ESRD at 12 months after diagnosis were recorded. The Birmingham Vasculitis Activity Score for Wegener’s granulomatosis (BVAS/WG)9 was calculated in all patients based on symptoms at presentation. Renal involvement was defined as either kidney biopsy-proven AAV or renal involvement in accordance with the BVAS/ WG. The patient’s medical records were reviewed for complete screening for renal involvement within two weeks before or after the diagnosis of AAV. Complete screening for renal involvement was defined in accordance with the Dutch guideline ‘Diagnostics of small-vessel vasculitis’14: assessment of serum creatinine and assessment of erythrocyturia and assessment of proteinuria. Proteinuria was defined as ≥ 500 mg/24 hours in accordance with proteinuria in the Vasculitis Damage Index.17 Erythrocyturia was defined as ≥ 10 red blood cells/high power field, in accordance with the BVAS/WG.9 Renal impairment was defined as serum creatinine ≥ 125 µmol/l, in accordance with BVAS version 3.18 All samples of serum creatinine and urine analysis three months prior to the biopsy were recorded in patients with renal biopsy-proven AAV.
Statistical analysis
The characteristics of patients who received complete screening for renal involvement within two weeks were compared with characteristics of patients without complete screening. A Wilcoxon signed-rank test was used to analyse the difference between serum creatinine at diagnosis and at 12 months in each group. In addition, renal outcomes defined as the development of ESRD and/or a rise in serum creatinine of > 30% at 12 months were compared between the two groups. The analysis was repeated with complete screening for renal involvement within four weeks instead of two weeks before or after the diagnosis of AAV. Chi-square tests, unpaired Student t-tests and Mann-Whitney’s U tests were used where appropriate. A p value < 0.05 was considered statistically significant. For data management and statistical analysis, Statistical Package for Social Sciences (SPSS®) version 20.0 was used.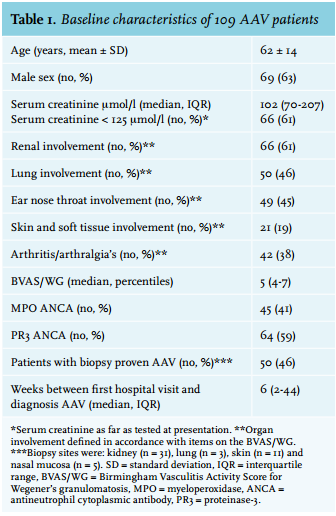
RESULTS
Between 1 February 2005 and 1 February 2015 a total of 239 patients tested positive for MPO or PR3 ANCA, of which 119 patients (50%) were diagnosed with AAV. The remaining 120 patients were diagnosed with inflammatory bowel disease (n = 24), other rheumatic diseases (n = 23), infection (n = 11), other (n = 29) or unknown (n = 2) diagnosis, or had unclassified symptoms (n = 31). After the exclusion of AAV patients who were diagnosed in a different hospital (n = 10), 109 patients were enrolled in this study. Patient characteristics are summarised in table 1. In short, the mean age was 62 ± 14 years and 63% were male. The median time between the first hospital visit with an AAV-related symptom and the diagnosis AAV was six weeks (interquartile range (IQR) 2-44).
Screening practice
In 90 of the 109 patients (83%) screening for renal involvement was completed within two weeks before or after the diagnosis. Of the 19 patients (17%) without complete renal screening: assessment of proteinuria was missing in all patients, urine sedimentation for erythrocyturia in 12 patients and serum creatinine in one patient. Screening in these patients was completed within four weeks in four patients, within two months in seven patients and within four years in three patients. In five patients, screening for renal involvement was not completed during a median follow-up of 2.2 years.
In comparison with patients with complete renal screening, patients with incomplete renal screening had a lower serum creatinine (median 70 (56-89) vs. 109 (74-248) µmol/l, p = 0.001) and a lower BVAS/WG (median 4 (3-7) vs. 5 (4-7), p = 0.03) (table 2). Notably, median BVAS/WG did not differ significantly after excluding erythrocyturia from the BVAS/WG.
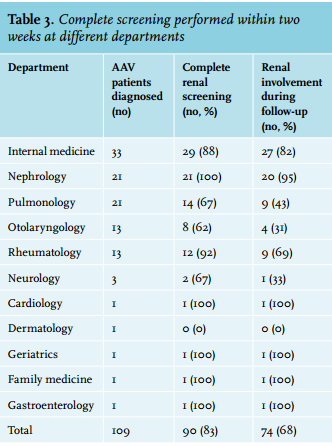
All patients (100%) diagnosed with AAV in the renal department had complete renal screening, as compared with 78% of patients who were diagnosed in other departments (p = 0.02, table 2 and table3). Of the 88 patients who were diagnosed with AAV in other hospital departments than the renal department, 54 patients (61%) developed renal involvement at any time during follow-up. Repeating the analysis using a cut-off for renal screening of four weeks instead of two weeks before or after the diagnosis yielded similar results.
Most patients with complete renal screening, (n = 72, 80%) were treated with a cyclophosphamide-based regimen for induction of remission. In patients without complete screening, seven patients (37%) were treated with a cyclophosphamide-based regimen (table 2). A total of 79 patients (73%) were treated with azathioprine and glucocorticoids for remission maintenance. 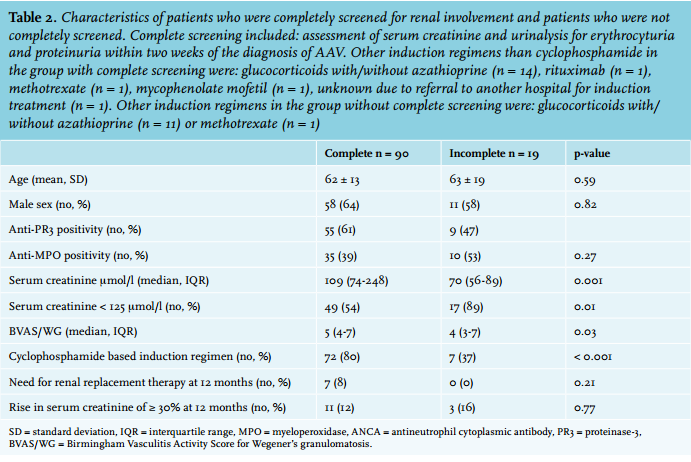
Renal prognosis
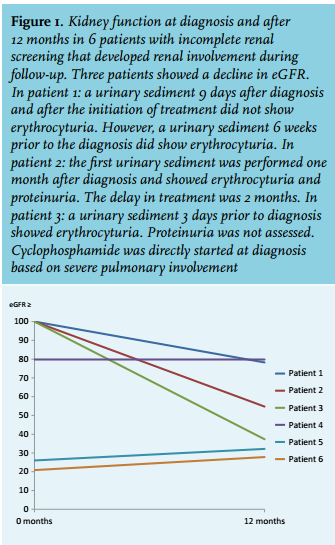
The median serum creatinine declined from 109 (74-248) to 103 (82-163) µmol/l in patients with complete screening (p = 0.20) and rose from 70 (56-89) to 81 (69-92) µmol/l in patients without complete screening (p = 0.65). None of the patients with incomplete renal screening developed ESRD. Of the 19 patients with incomplete screening, renal impairment or urinary abnormalities were documented in six patients at any point during a median follow-up of 5.2 years (2.1-9.7). Three of these patients had a decline in kidney function over the 12 months after diagnosis (figure 1). In all three patients the deterioration of kidney function coincided with erythrocyturia. In one patient the deterioration of kidney function coincided with proteinuria. Proteinuria was not assessed in the other two patients. In one patient there was a delay in treatment of two months. In the other two patients treatment was initiated at diagnosis. Of these three patients, one was treated with cyclophosphamide and two were treated with prednisolone induction therapy.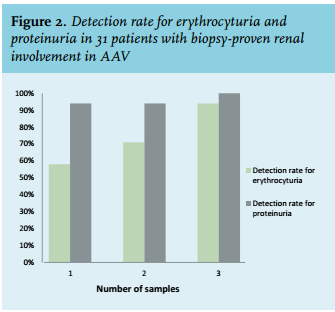
Laboratory findings in patients with kidney biopsy proven AAV
In 35 patients a kidney biopsy was performed, of which 31 were typical for AAV and four were inconclusive. The kidney biopsies were performed as part of the initial diagnostic process. The indication for a biopsy was established based on clinical decision, not on a standardised protocol. Of the 31 patients with kidney biopsy proven AAV, five (16%) did not have renal impairment. A median of three (2-4) urinary sediments were collected and examined for erythrocyturia in the three months preceding the biopsy. Results from these urine analyses were variable within these patients. In 18 of the 31 patients (58%), all urine samples showed erythrocyturia. Three samples were required to detect erythrocyturia in 94% of patients (figure 2). In 29 of 31 patients proteinuria was detected in all samples (figure 2). The number of required samples for the detection of erythrocyturia or proteinuria was not related to kidney function.
DISCUSSION
In this cohort of AAV patients from a teaching hospital in the Netherlands, screening for renal involvement was performed in 83% of AAV patients within two weeks before or after the diagnosis. Patients with normal kidney function and patients who presented outside the renal department were at risk of incomplete screening for renal involvement, which may ultimately lead to kidney function loss. In three patients with incomplete screening for renal involvement, kidney function decreased in the year after diagnosis; two of these patients were not treated with appropriate immunosuppressive induction therapy covering renal involvement. Unawareness of renal involvement may have played a role in the choice for the type of immunosuppressive agents in these patients and therefore may have contributed to the kidney function loss. The question arises whether all AAV patients require full renal screening. Although the clinical course of patients with AAV is variable, in most patients the acute phase of systemic vasculitis is preceded by a phase with more mild symptoms.11,19 During this phase of the disease, many patients suffer from upper respiratory complaints and arthralgia. Patients then usually progress to a more acute phase of the disease, in which rapidly progressive renal failure is a common feature.5,19 Unfortunately, if renal involvement is diagnosed too late, some patients will have already developed severe kidney damage, occasionally with the need for renal replacement therapy.5,10 In our cohort 61% of AAV patients who were diagnosed outside the renal department developed renal involvement at any time during follow-up. This indicates the high occurrence of renal involvement in AAV patients who present with other than renal symptoms and emphasises the necessity of complete and repeated renal screening in all patients.
Early screening for renal involvement may have considerable clinical implications. So far randomised controlled studies have not assessed the benefit of aggressive immunosuppressive therapy specifically in patients with early renal disease without loss of renal function. However, observational studies suggest that patients with urinary abnormalities but preserved renal function benefit from aggressive treatment. As already briefly mentioned in the introduction, Hanaoka and colleagues studied 27 patients with biopsy-proven renal involvement, of which 12 patients had preserved eGFR. These patients were divided into two groups according to intravenous cyclophosphamide exposure. At three-year follow-up, patients without cyclophosphamide treatment had significantly lower eGFR than those with cyclophosphamide treatment (42.1 vs. 62.1 ml/min/1.73 m2 , p = 0.01).11 It is therefore suggested that when patients with renal AAV and urinary abnormalities but a preserved eGFR are treated with aggressive immunosuppressive therapy, irreversible damage due to glomerulonephritis can be prevented.2,11,13 Apart from the direct therapeutic implications of renal screening, renal baseline parameters also serve the interpretation of future laboratory variables. Current guidelines recommend urine analysis at each patient visit in order to screen for a possible renal relapse or therapy toxicity.6,20 Knowledge on the course of erythrocyturia (new onset/decreasing) enhances comprehension of disease activity and can guide clinical decision-making.
Based on our findings, we agree with the Dutch guideline ‘Diagnostics of small-vessel vasculitis’14 that screening for renal involvement should include serum creatinine and urine analysis for both erythrocyturia and proteinuria, early in the diagnostic process. In addition, we found that a higher sensitivity for erythrocyturia is achieved if urine sediments are repeated up to three times. Urinary abnormalities in AAV with a preserved renal function require a renal biopsy in order to determine renal involvement. If a renal biopsy confirms renal involvement of AAV, aggressive immunosuppressive agents are indicated. Screening for renal involvement in the diagnostic process of AAV may serve two purposes. First, if erythrocyturia, proteinuria or a rise in serum creatinine are present, this may support the diagnosis of AAV. Second, if AAV is diagnosed based on other findings, screening for renal involvement establishes the extensiveness of the disease and may guide the choice of therapy.2,8,11 If AAV is suspected in patients outside the internal medicine/nephrology/rheumatology department, early consultation of a physician with expertise in the field of nephrology is suggested.
To our knowledge, this is the first study evaluating the adequacy and reproducibility of screening for renal involvement in AAV patients in clinical practice. Hence, it is unknown to what extent these results would apply to other centres. However, the presence of renal involvement in our population seems consistent with previous reports.3,4 Furthermore, the number of patients with biopsy proven renal vasculitis (n = 31) in our study was relatively low. However, previous studies found comparable laboratory findings preceding renal biopsy-proven AAV.21,22 In this study the median BVAS/WG was 5.0 (4-7) (mean 5.8 ± 2.8).
These results were slightly lower than in the Rituximab in ANCA-Associated Vasculitis (RAVE) trial (mean 8.5 ± 3.2) and in the Wegener’s Granulomatosis Etanercept Trial (WGET) (mean 6.9 ± 3.4).23,24 These higher scores could be explained by study selection criteria in the RAVE trial: an indication for cyclophosphamide and BVAS/WG ≥ 3. Furthermore, the slightly higher BVAS/WG in these trials may be due to the prospective collection of data. Although the historical patient files were of high quality, the retrospective design of our study may account for an information bias on documented symptoms and in some cases the exact date of the diagnosis.
In conclusion, in this cohort screening for renal involvement was performed within two weeks of the diagnosis in the majority of AAV patients. However, especially in patients with normal eGFR and a first presentation to other departments than the renal department, there may be room for improvement. These results suggest that a multi-disciplinary collaboration is warranted for an optimal diagnostic process. More awareness for the clinical features of renal involvement in AAV is a key element in the prevention of irreversible kidney damage.
DISCLOSURES
All authors declare no conflicts of interest.
REFERENCES