KEYWORDS
ACTH stimulation test, adrenal insufficiency, low dose synacthen test, morning cortisol
INTRODUCTION
The measurement of serum morning cortisol concentration is an appropriate and practical first-line screening test for adrenal insufficiency.1 Upper and lower cortisol cut-off values are used to differentiate between low levels (where adrenal insufficiency can be diagnosed without further dynamic hypothalamic-pituitary-adrenal (HPA) axis testing), intermediate levels (where dynamic testing is needed to confirm or reject the diagnosis), and high levels (where the diagnosis can be safely rejected without additional testing).
Several factors influence the interpretation of the serum cortisol level. Firstly, most assays that are used for determining the serum cortisol concentration measure the total cortisol concentration. This consists of the concentrations of free cortisol, cortisol bound to corticosteroid-binding globulin (CBG) and cortisol bound to albumin.2,3 Because of this, elevated concentrations can be found when CBG is increased by oestrogen therapy, or decreased concentrations can be found when CBG is reduced in liver diseases such as cirrhosis.4,5 Furthermore, the measured cortisol level varies between different cortisol assays, making it difficult to set morning cortisol cut-off values that can be generally applied.4,6
The generally accepted lower and upper cut-off values of morning cortisol are 100 nmol/l and 500 nmol/l, respectively.1,7 However, reported lower cortisol cut-off values range from 80 nmol/l to 165 nmol/l and reported upper morning cortisol levels range from 236 nmol/l to 500 nmol/l.7-20 This variability may in part be due to the difference in the cortisol assays used. Also, these reported values are defined by their sensitivity and specificity to predict the outcome of different dynamic ACTH tests. In most studies reporting morning cortisol criteria, the cut-off values are related to the outcome of the insulin tolerance test. In newer studies, the cut-off values are related to the high-dose (250 µg) short synacthen test. Interestingly, we could not find reported morning cortisol cut-off values directly related to the outcome of the low-dose (1 µg) short synacthen test (LD-SST).
Multiple meta-analyses have been performed comparing high- and low-dose ACTH stimulation tests.21-23 Two meta-analyses report similar diagnostic performance of the two tests and one reports a better performance of the low-dose test. Several studies have shown that the LD-SST is more sensitive for diagnosing mild or recent-onset central adrenal insufficiency.24-35
The LD-SST is a suitable and frequently used dynamic test for diagnosing adrenal insufficiency. Nevertheless morning cortisol cut-off values related to the LD-SST are lacking. The aim of this study is to provide these cut-off values and to identify other variables that can be used to predict the outcome of the LD-SST.
MATERIALS AND METHODS
Patients
Data of all patients who underwent an outpatient LD-SST in our hospital from January 2003 to March 2015 were collected retrospectively. Only the first LD-SST in this period was included when more than one test was performed per patient. All tests of which a morning cortisol measurement up to three months prior to the LD-SST was known were identified. Morning levels were defined as samples taken between 7:00 and 9:00 am. According to protocol, glucocorticosteroids must be discontinued at least 24 hours prior to the LD-SST. However, due to the retrospective nature of this study it cannot be ascertained that all patients were thus instructed by their referring physician.
Materials and definitions
LD-SSTs were carried out between 8:00 am and 17:00 pm. All tests were performed by a small group of well-trained medical personnel. Patients received an indwelling intravenous catheter. At t = 0 a venous blood sample was taken. Subsequently a 1 µg bolus of synthetic ACTH1-24 (Synacthen®) was administered intravenously. The 1 µg solution was freshly prepared by diluting a 250 µg ampoule of tetracosactide (Novartis Pharma, Nurnberg, Germany) in normal saline (final volume 0.5 ml). The syringe was flushed with 1 ml of normal saline to ensure complete intravenous injection of the 1 µg solution. After 30 minutes venous blood samples were taken for cortisol measurement. The outcome of the LD-SST was considered normal if cortisol levels at either t = 0, t = 30 or t = 60 were higher than 500 nmol/l. The outcome of the test was considered abnormal if cortisol levels were below 500 nmol/l in all samples.
Hormone analysis
All serum cortisol samples were analysed in a solid-phase competitive chemiluminescence enzyme immunoassay using the Immulite 2000 platform (Siemens Medical Solutions Diagnostics, Los Angeles, CA). The intra- and inter-assay coefficients of variation of the cortisol assay are < 10%.
Data collection and definitions
For each patient, morning cortisol concentration prior to the test (if known), use of glucocorticosteroids, history of autoimmune diseases and the main reason for performing the LD-SST were recorded. These reasons were divided into five categories: chronic fatigue symptoms, chronic fatigue in combination with a history of thyroid disease, symptoms of orthostasis or hypotension, suspected pituitary pathology and all other reasons. Only autoimmune diseases associated with autoimmune polyglandular syndrome (APS) type 1, 2 and 4 in the patient history were recorded: diabetes mellitus type 1, hypoparathyroidism, mucocutaneous candidiasis, pernicious anaemia, hypothyroidism, Graves’ disease, Hashimoto’s thyroiditis, coeliac disease, primary hypogonadism, alopecia, vitiligo, autoimmune hepatitis and chronic gastritis.36 Additionally, pregnancy or oestrogen therapy during testing and history of liver diseases were recorded. Also the final diagnosis as documented by the physician after interpretation of the LD-SST and any additional tests was recorded.
Statistical analysis
For determining upper and lower morning cortisol cut-off values, receiver operator characteristic (ROC) curve analysis was performed. The predictive value of the different predictor variables was tested by univariable and multivariable binary logistic regressions. Firstly, all the predictor variables were analysed using univariable binary regression models. Subsequently, all predictors with a p-value higher than 0.200 were included in a multivariable binary regression model. Stepwise, the predictor with the highest p-value was excluded from the model until the model consisted of only statistically significant predictors, p < 0.05. We adhered to the ‘events per variable’ rule to ensure adequate power in the logistic regression analyses.37 All statistical analyses were performed with SPSS version 22 for Windows.
RESULTS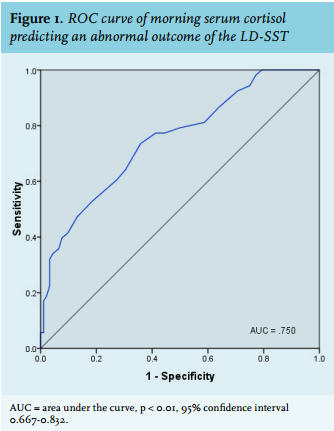
Morning cortisol cut-off values
For determining optimal upper and lower cortisol cut-off values, a ROC curve was used (figure 1). Including only the outpatient LD-SSTs of which a morning cortisol level prior to the test was known, 145 tests and corresponding morning cortisol measurements were analysed. The area under the curve was 0.750 (95% CI 0.66-0.832, p = 0.000). The optimal lower cut-off value of morning cortisol was set at a point that ensured identification of all abnormal LD-SSTs, having the highest specificity and the highest positive predictive value. The optimal upper morning cortisol value was set at a point that ensured identification of all normal LD-SSTs, having the highest sensitivity and the highest negative predictive value (table 1).
In this sample there was one patient with an immeasurably low morning cortisol level and nonetheless a normal LD-SST. This low morning cortisol level was possibly due to a measurement error. Also, the basal cortisol measurement in the LD-SST of this patient (performed at 9:20 am) was 310 nmol/l. The optimal lower cut-off value of morning cortisol was set at 145 nmol/l. If the data of this one patient were included in the analysis, the specificity and positive predictive values were 89.9% and 90.0%, respectively. If this patient was excluded from the analysis, however, both specificity and positive predictive value were 100%. The optimal upper cut-off value was set at 375 nmol/l, with 100% sensitivity and 100% negative predictive value. 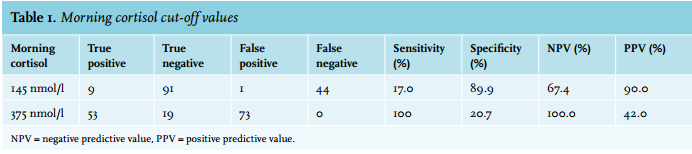
OTHER PREDICTOR VARIABLES OF THE LD-SST
A prediction model was fitted using univariable and multivariable binary logistic regression analysis of the defined predictor variables. Due to the small number of patients in this sample group, only two variables other than morning cortisol concentration could be included in a statistically significant prediction model.
The number of analysed tests was increased by also including the LD-SSTs without a morning cortisol measurement prior to the test. All LD-SSTs performed in an outpatient setting from January 2010 to March 2015 were analysed, resulting in a sample of 329 patients. Patient demographics are summarised in table 2. The average age was 47 years. There was no significant difference between the ages of patients with a normal or an abnormal outcome of the LD-SST (Mann-Whitney test, p = 0.154). A total of 76 tests (23.1%) were abnormal.
The final prediction model of the LD-SST showed a significant predictive value of a history of autoimmune diseases associated with APS, use of glucocorticosteroids, fatigue symptoms and symptoms of hypotension (table 3). Notably, 39.5% of the 38 patients that used glucocorticosteroids had an abnormal LD-SST.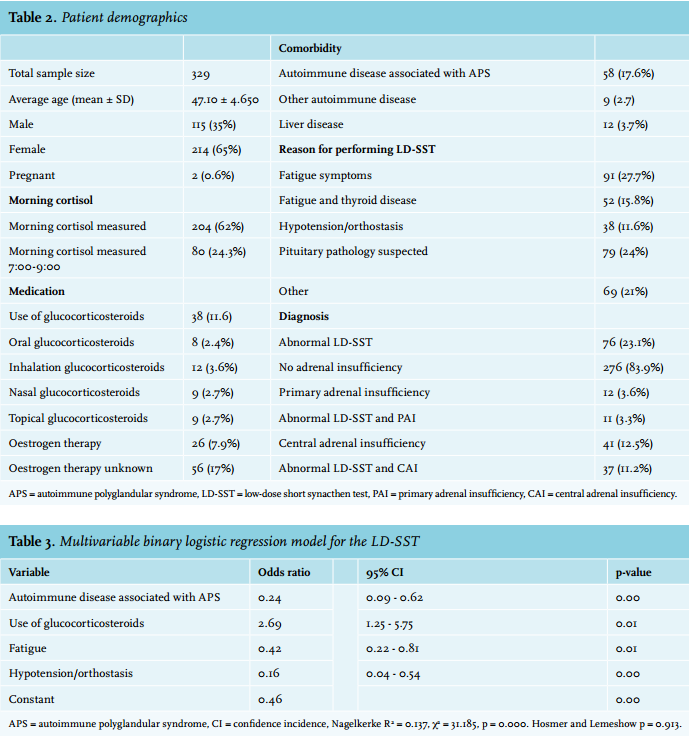
Predictors of central adrenal insufficiency
As shown in table 2, nearly half of the patients with abnormal LD-SSTs are ultimately diagnosed with central adrenal insufficiency and only 14.5% of patients with abnormal tests are diagnosed with primary adrenal insufficiency. We hypothesised that the use of glucocorticosteroids would be a stronger predictor when a priori central adrenal insufficiency is suspected. A second predictor model was fitted for predicting central adrenal insufficiency (table 4). Because only 12 patients were diagnosed with primary adrenal insufficiency, no multivariable predictor model for this diagnosis could be developed based on the ten events per predictor variable rule. 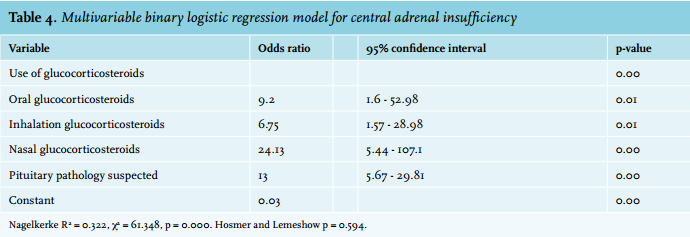
DISCUSSION
Morning cortisol cut-off values
Only a small number of LD-SSTs performed in an outpatient setting have an abnormal outcome. In our sample, only 23.1% of the tests were abnormal. We hypothesised that the number of unnecessarily performed tests could be safely reduced, primarily by determining morning cortisol cut-off levels specifically related to the LD-SST.
We could find no such cut-off values in the current literature, since all research done regarding morning cortisol and its relation to dynamic ACTH-axis testing is related to either the insulin tolerance test or the high-dose short synacthen test.7-20 These data have been extrapolated to the LD-SST without supporting evidence in the literature.
Based on a ROC analysis of morning cortisol measurements in 145 subjects, a lower morning cortisol concentration of 145 nmol/l and an upper morning cortisol concentration of 375 nmol/l were identified as optimal cut-off values using the Immulite 2000 cortisol assay. By using these new cut-off values instead of conventional cut-off values of 100 nmol/l and 500 nmol/, the number of justified LD-SSTs would be reduced by 12% based on our data sample.
OTHER PREDICTOR VARIABLES OF THE LD-SST
The second hypothesis was that other than only morning cortisol concentrations, additional predictors could be used to identify patients with an abnormal LD-SST. As expected, a normal outcome of the LD-SST was more likely when the main reason for performing the test was chronic fatigue or symptoms of orthostasis. When there are no other supportive arguments for adrenal insufficiency than these symptoms, performing the LD-SST should be reconsidered.
Also as hypothesised, the use of glucocorticosteroids predicted an abnormal outcome of the LD-SST. Chronic use of glucocorticosteroids is one of the most common causes of central adrenal insufficiency, other common causes being pituitary processes and iatrogenic causes after pituitary surgery or radiation therapy. A meta-analysis by Broersen et al. shows that development of adrenal insufficiency can occur in up to 60% of patients using glucocorticosteroids, depending on the route of administration, dosage and duration of use.38
In our study, 13% of 37 patients with an abnormal LD-SST who were diagnosed with central adrenal insufficiency used glucocorticosteroids. Most patients with central adrenal insufficiency had a pituitary tumour or pituitary surgery (59.5%). Other causes were Sheehan’s syndrome (5.4%) or unknown (21.6%). These results underline that other than pituitary processes or surgery, glucocorticosteroid use is a common cause of central adrenal insufficiency.
On a side note, although glucocorticosteroid use was considered the cause of central adrenal insufficiency in a large number of patients, the chronic use of glucocorticosteroids in itself was rarely the reason for performing the LD-SST in our population. Fatigue symptoms and suspected pituitary pathology were the most common reasons for performing the test (table 2).
Analysis of different routes of administration of glucocorticosteroids in our study did not provide significant results. However, when analysed for predicting the final diagnosis of secondary adrenal insufficiency, the use of oral, inhalation and nasal glucocorticosteroids were all significant predictors. We therefore suggest that not only oral administration, but also inhalation and nasal administration of glucocorticosteroids can be used as a supportive argument for performing the LD-SST.
Inhaled glucocorticosteroids are known to have systemic steroid activity. A recent systemic review reports HPA suppression resulting in suppressed urinary cortisol, depending on the type of inhaled glucocorticosteroids used.39 Multiple studies show no suppressing effect of nasal glucocorticosteroids on the HPA axis and dynamic stimulation tests, in a maximum treatment period of four weeks.40,41 The effects of long-term use of nasal glucocorticosteroids on ACTH stimulation tests, however, remain unclear.
Three variables that might interfere with measured cortisol levels were also included in the analysis, namely pregnancy or oestrogen therapy during testing and a history of liver disease. None of these variables were significant predictors in the final model. Nevertheless, oestrogen therapy was a marginally significant predictor of the LD-SST when analysed using univariable binary logistic regression. Its predictive value might be stronger than we found, because in 26.2% of all females the use of oestrogen therapy during testing was unknown. This illustrates that often this variable is overlooked when diagnosing adrenal insufficiency.
In the literature, a two- to three-fold elevation of CBG concentration has been observed in women using oral contraceptives, leading to concordantly elevated morning and stimulated cortisol levels in ACTH stimulation tests.4 Although oestrogen therapy was not a significant addition to the final model in our study, it does appear to be an important factor. Oral contraceptives should be discontinued before the LD-SST is performed or specific cut-off levels should be used. Also, the use of oral contraceptives should be taken into account when interpreting a screening morning cortisol measurement.
Unexpected results
In the final predictive model for an abnormal LD-SST, a history of autoimmune diseases associated with APS predicted a normal outcome. This was the opposite of what was expected. We hypothesised that primary adrenal insufficiency and therefore an abnormal LD-SST would be more likely. This unexpected result could be explained by the relatively small number of patients with an abnormal LD-SST and final diagnosis of primary adrenal insufficiency in the sample group. In our sample group this was the case in only 3.3% of the subjects, compared with 11.2% of the subjects where the LD-SST was abnormal and central adrenal insufficiency was diagnosed. Autoimmune diseases are not associated with central adrenal insufficiency. Also the a priori chance of primary adrenal insufficiency is small, the incidence in Europe is 4.4-6.0 per million per year.1 It could be that in patients with a history of APS-associated autoimmune disease, it is more likely that their symptoms have a different aetiology than adrenal insufficiency. It seems that such a patient history does not make an abnormal LD-SST more likely.
Limitations
Of all the LD-SSTs performed in an outpatient setting in our hospital between 2003 and 2015, there is a relatively small number of tests where a morning cortisol level prior to the test was known. For this reason it was not possible to make a predictive model for the outcome of the LD-SST, which included morning cortisol as a predictive variable. Such a model would have better identified variables that have a predictive value in addition to morning cortisol itself.
Another limitation is the small number of patients that are diagnosed with primary adrenal insufficiency in this study. One of the consequences is the unexpected result of an abnormal LD-SST being less likely when there is a history of APS-associated autoimmune disease. By extension, the final predictor model could be considered better suited for when central adrenal insufficiency is suspected compared with a suspected primary adrenal insufficiency. However, this study was designed to identify predictors of the outcome of the LD-SST regardless of the incidence of primary and central adrenal insufficiency. In this study we cannot extrapolate the results to patients with suspected primary adrenal insufficiency because of the small number of patients with this diagnosis.
The binary logistic regression model of this study was built with data which were collected retrospectively. More research should be done to verify this model in a prospective setting, including a morning cortisol measurement prior to the LD-SST in all subjects.
CONCLUSION
The number of low-dose synacthen tests performed in an outpatient setting can be safely reduced by altering the conventional cut-off values of screening morning cortisol measurements. We propose an upper cut-off value of 375 nmol/l and a lower cut-off value of 145 nmol/l. A normal outcome is more likely when the main reasons for performing the test are fatigue symptoms or hypotension. An abnormal outcome is more likely when glucocorticosteroids are used. Especially when central adrenal insufficiency is suspected, different routes of administration of glucocorticosteroids should be taken into account.
DISCLOSURES
The authors have no conflicts of interest to disclose.
REFERENCES