KEYWORDS
VTE, D-dimer, pulmonary embolism, cancer
INTRODUCTION
D-dimer is a degradation product of cross-linked fibrin and is routinely used in diagnostic algorithms for venous thromboembolism (VTE).1 Since in such algorithms, the D-dimer is exclusively used as part of a rule-out strategy, a low cut-off value has been chosen to generate a highly sensitive dichotomous test for diagnosing VTE.2 Indeed, in both deep vein thrombosis (DVT) and pulmonary embolism, the commonly used cut-off value (500 µg/l) is associated with a high sensitivity which, combined with a low probability of VTE based on a clinical decision rule (such as the Well’s Score), effectively rules out clinically significant VTE. This strategy is now firmly established in national and international guidelines and routine practice.3 Among clinicians, a positive D-dimer test has a reputation of being very non-specific for VTE or in fact for any other disease. It is important, though, to acknowledge that tests that generate results on a continuous scale have no intrinsic sensitivity or specificity: only results above or below a chosen threshold have such properties.4 In general terms, and as illustrated by receiver operating characteristic curves, the more abnormal a test result becomes, the higher its specificity. Previous studies on the magnitude of D-dimer elevation mainly focussed on the positive predictive value for diagnosing VTE. Limited data from such studies indeed suggest that with higher D-dimer values, VTE becomes more likely.5-7 However, which conditions other than VTE may cause sharply elevated D-dimer levels is less well established. It is also unknown how often sharply elevated D-dimer levels occur without evidence of underlying disease. The latter is particularly relevant when no diagnosis is as yet apparent, and discharge or outpatient follow-up may be considered. Knowing that D-dimers reflect fibrinolysis, we hypothesised that extremely elevated D-dimers are almost universally associated with either VTE or with other conditions known to be associated with activation of coagulation, such as sepsis or cancer. Hence, we anticipated that in the vast majority of cases of sharply elevated D-dimer levels, there is an associated clinical condition that requires further investigation or (urgent) medical treatment.
METHODS
Study design and patient selection
We performed a retrospective cohort study of patients with an extremely elevated D-dimer, which we arbitrarily defined as more than 10 times the commonly used cut-off value of 500 µg/l. All D-dimer results > 5000 µg/l, between 1 January 2004 and 31 December 2012, were obtained from the laboratory database of our hospital, which is a large secondary and tertiary care facility. Patients ≥ 18 years were eligible regardless of whether they were outpatients, admitted patients, or patients presenting via the emergency department. In our hospital, the routine indication for ordering D-dimer is to rule out VTE (at a fixed cut-off of 500 µg/l), but in daily practice, many physicians do not order D-dimer measurement as part of a formal VTE diagnostic strategy. D-dimer values were determined using a standardised immune-turbidimetry assay (Modular P800, Roche diagnostics). Besides D-dimer, concomitant leucocyte, platelet, coagulation and C-reactive protein results were retrieved, if available. Patients who underwent cardiopulmonary resuscitation (CPR patients) were excluded. The STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines were followed where possible.8
Data collection and analysis
Electronic medical records were reviewed for the primary diagnosis. If multiple diagnoses were recorded, all were included in the database. Furthermore, pregnancy and known cancer were registered. If imaging modalities were used following D-dimer testing, the results were registered. All diagnoses were categorised into predefined major disease groups (table 1). One-way ANOVA was used to compare coagulation parameters in tertiles of D-dimer levels. A p-value of ≤ 0.05 was considered to indicate statistical significance. 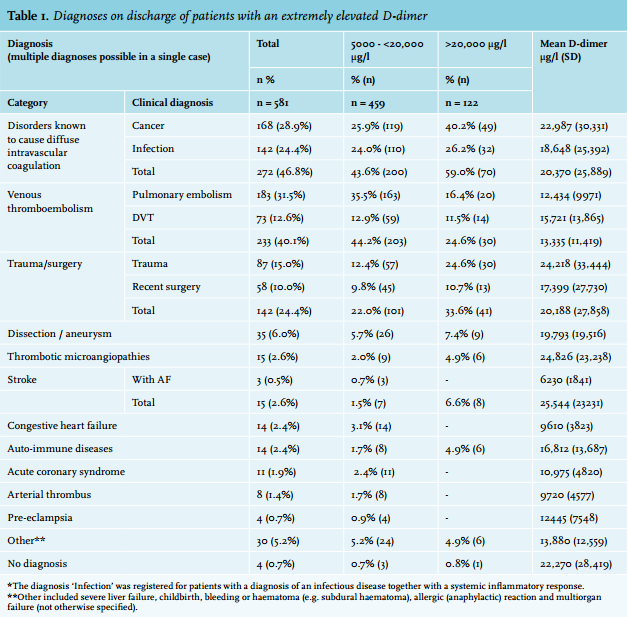
Ethical considerations
Formal ethical approval of the VU University Medical Center ethics review board was not necessary, as this study does not fall under the scope of the Dutch Medical Research Involving Human Subjects Act (WMO).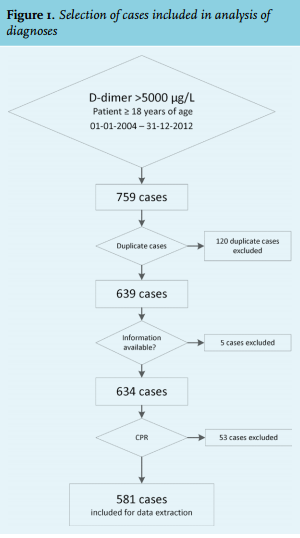
RESULTS
Patient characteristics
A total of 759 extremely elevated D-dimer values (> 5000 µg/l) were identified. An inclusion flow diagram is shown in figure 1. After exclusion of 120 duplicate cases, 53 CPR patients, and 5 patients without clinical information in the medical records, 581 cases (295 male, 286 female, mean age 62 years, SD 19) were included. The D-dimer range of included patients was 5030 µg/l to 239,000 µg/l, with a mean of 17,597 µg/l (SD 22,972 µg/l). Pulmonary CT angiography was performed in 299 patients (51.5%), in 28 (4.8%) ventilation-perfusion scintigraphy was performed, and in 95 patients (16.4%) leg compression ultrasonography was done.
Venous thromboembolism, cancer and sepsis account for the majority of diagnoses
In 577 patients (99.3%) a primary diagnosis was registered, and in 252 patients (43.3%) one or more secondary diagnoses were also established. No diagnosis was registered in only four cases. The most frequent diagnoses are displayed in table 1. Almost one-third of all patients were diagnosed with pulmonary embolism. Combined with the DVT cases (12.6%) they were categorised as VTE, which accounted for just over 40% of all patients; 168 patients (28.9%) were diagnosed with cancer, which was the second most common diagnosis. Severe infection/ sepsis was the third most frequently encountered diagnosis, established in 142 patients (24.4%).
Trauma or surgery was the prime diagnosis in 142 patients, but was frequently complicated by a second diagnosis, as 15.5%, 15.5% and 14.8% of them additionally had VTE, cancer or sepsis/infection, respectively. A total of 79 patients with sharply elevated D-dimers had surgery/ trauma as a single diagnosis.
In the 233 patients diagnosed with VTE (DVT or pulmonary embolism), 69 (29.6%) had a concurrent diagnosis of cancer. We observed more malignancies in the VTE cases with a D-dimer ≥ 20,000 µg/l (n = 15/30, 50.0%) compared with VTE patients with a D-dimer between 5000 and 20,000 µg/l (n = 54/203 26.6%), (chi-square, p = 0.009).
Other diagnoses
In 11.5% of cases, no VTE, sepsis, cancer and/or trauma/ surgery was diagnosed. Among these, the most frequent diagnoses were aortic dissection/aneurysm (6.0%), and stroke (2.6%). All other clinical diagnoses were less frequent than 2.5% (table 1). The 5.2% of diagnoses classified as ‘other’ in table 1 occurred in two patients or less and included, among others, liver failure, childbirth, bleeding or haematoma (e.g. subdural haematoma), allergic (anaphylactic) reaction and multiorgan failure (not further specified). Pregnancy, a condition known to contribute to elevated D-dimer levels, was present in 25 cases (4.3%). In all pregnant patients a second diagnosis was noted, being pregnancy related (i.e. pre-eclampsia, HELLP, or childbirth) or with another diagnosis in the table.
Fourteen patients were diagnosed with heart failure, which we believe is unlikely to contribute significantly to such a D-dimer elevation in cases that are otherwise uncomplicated.
Many patients with sharply elevated D-dimers have additional signs of activated coagulation
Table 2 shows the results of haemostatic variables. Over one-third of the studied patients had concurrent thrombocytopenia (thrombocyte count < 150 x 109) and over half of the patients had a prolonged coagulation time (prothrombin time > 1.20 INR, or activated partial thromboplastin time; aPTT > 40 sec). Haemostatic variables were generally more indicative of diffuse intravascular coagulation (DIC) in the highest tertile of D-dimer levels. 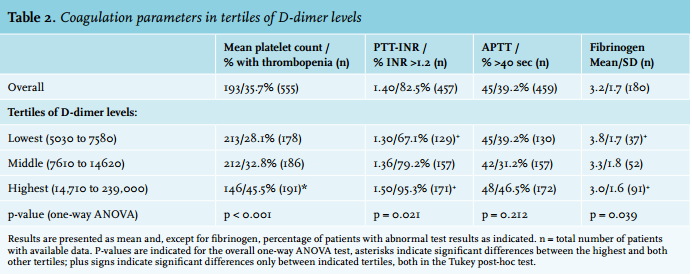
DISCUSSION
The salient finding of our study is that a sharply elevated D-dimer level, arbitrarily defined as > 5000 µg/l, has a very high predictive value for serious disease, mainly including VTE, sepsis and cancer. Even in the patients with VTE, underlying cancer was more prevalent in the highest D-dimer ranges. If the cause of an extremely elevated D-dimer is not immediately apparent during initial clinical evaluation because patients may not appear seriously ill, suspicion of serious underlying disease should persist. The most common diagnoses were VTE (40.1%), sepsis (24.4%), cancer (28.9%), and complicated trauma/surgery (24.4%). In clinical practice, VTE and sepsis are unlikely to be missed if such extreme D-dimer results are found, because suspicion of VTE is commonly the clinical indication for D-dimer testing in the first place, and sepsis is usually evident on clinical grounds. However, some cases of sepsis and many cases of cancer may not be evident clinically, and extreme D-dimer levels in patients without VTE or manifest sepsis should thus alert clinicians to the possibility of these diagnoses. In addition, sharply elevated D-dimer levels more rarely point to other conditions that may be difficult to diagnose, particularly in an acute setting, such as aortic dissection. In any case, our results suggest that virtually all patients with sharply elevated D-dimer levels have one or multiple serious conditions. Clinicians may regularly encounter patients who are, for example, suspected of having pulmonary embolism, have an extremely elevated D-dimer level but negative results on CT angiography. The results of our study encourage careful evaluation of other causes of such extreme D-dimer levels, rather than disregarding them because ‘D-dimer is a non-specific test’.
Previous studies on the magnitude of D-dimer elevation mainly focussed on the positive predictive value specifically for diagnosing VTE, and also suggested that the magnitude of D-dimer elevation correlates with the likelihood of having VTE. One study found pulmonary embolism in 35.3% of 34 patients with a D-dimer of 5000 to 20,000 µg/l and in 45.5% of only 11 patients with a D-dimer of > 20,000 µg/l.5 A second study concluded that infection, sepsis and cancer should be considered in patients with elevated D-dimer above the regular cut-off level of 500 µg/l.9 In this study the prevalence of cancer and infection/sepsis was 6.3% and 35.9%. This study, however, did not address prevalence for extremely elevated D-dimer levels, such as we present here.
Mechanistically, sharply elevated D-dimer levels must reflect widespread activation of the coagulation and subsequent fibrinolysis cascades. This can occur either locally (as in VTE or arterial calamities, such as dissection or arterial thrombosis) or diffusely. Indeed, many patients in our cohort suffered from conditions such as sepsis and cancer, known to trigger widespread activation of coagulation. These patients also showed a profile of other haemostatic parameters (platelet count, plasmatic coagulation tests) compatible with DIC, particularly in the highest tertile of D-dimer levels. However, an explicit clinical diagnosis of DIC was established in only 5.2% of patients in this study. This may largely be a matter of definition and classification, the formal criteria for diagnosing diffuse intravascular coagulation being chosen to generate a relatively high threshold for establishing the diagnosis, excluding mild to moderate coagulation activity, coagulation factor deficiency or low platelet counts due to other causes. D-dimer is one of the criteria to diagnose (overt) DIC together with fibrinogen, aPTT and platelet count,10,11 and sharply elevated levels in particular strongly contribute to the diagnosis of DIC by consensus criteria.12,13 The optimal cut-off levels of D-dimer for diagnosing DIC vary between 3000 and 4000 µg/l.14,15
One of the conditions known to cause diffuse intravascular coagulation activity is cancer.12,16 In our cohort, a very high D-dimer was associated with the presence of cancer. Almost one-third of our patients with a VTE had cancer, and in the cases with a D-dimer > 20,000 µg/l the prevalence of diagnosed cancer was no less than 40%. However, cancer was also diagnosed in a substantial number of patients without VTE. The association between D-dimer elevation and cancer has been described earlier, both in non-VTE and in VTE patients.17-19 In cancer patients without VTE, the degree of D-dimer elevation has been associated with survival.19,20 In patients with VTE, the incidence of cancer during follow-up was twice as high in those with D-dimer levels > 4000 µg/l.21 In another study, 27.5% of patients with a D-dimer level > 8000 µg/l (n = 40) had, or developed cancer.19 Taken together, these studies support the notion that sharply elevated D-dimer levels should trigger the suspicion of cancer, both in VTE and non-VTE patients.
Other diagnoses than VTE, sepsis or cancer may also explain sharply elevated D-dimer levels. These diagnoses, listed in table 1, may often be evident from history taking and routine physical examination, but others may be harder to diagnose. Among the former are trauma and recent surgery. Previous studies also suggested that D-dimer levels may be correlated with the severity of trauma.22,23 Among the diagnoses that can be missed are for example pregnancy, which may be denied or unknown to patients, and the ones that are notably difficult diagnoses such as aortic dissection and thrombotic microangiopathy. Although such diagnoses are rare, even in our group with extremely elevated D-dimer levels, clinicians should consider them if no other causes are apparent. Even in pregnant patients their pregnancy was ‘just’ a contributing factor to the elevated D-dimer levels, it was always complicated by other diseases in this sharply elevated D-dimer study.
Several limitations of this study merit consideration. We retrospectively identified causes of sharply elevated D-dimer levels from the medical records. A prospective, protocolised diagnostic work-up may have yielded different diagnoses. Also, disease severity and the added value of the D-dimer result in establishing a diagnosis could not be systematically assessed retrospectively from patient files. Finally, results could be different in other types of hospitals, and almost certainly will be different in primary care facilities, where the prior likelihood of severe disease is lower.
In conclusion, an extremely elevated D-dimer is specific for serious illness and should trigger suspicion of severe disease, particularly VTE, sepsis or cancer, the last of which even in the presence of VTE. In patients not appearing seriously ill, physicians are ill-advised to ignore such results based on a presumed lack of specificity of the D-dimer test. Further studies should define the optimal diagnostic work-up of an extremely elevated D-dimer.
ACKNOWLEDGEMENTS
The authors would like to thank Monique Terwijn and the Department of Clinical Chemistry of the VU University Medical Center for providing the laboratory data and the department heads of the VU University Medical Center for giving consent to perform this study.
DISCLOSURES
The authors declare that they have no conflict of interest.
REFERENCES