KEYWORDS
Chronic pericarditis, Coxiella burnetii, recurrent pericarditis 
INTRODUCTION
In over 80% of cases, acute and recurrent pericarditis remains aetiologically unexplained. Even with a very extensive diagnostic examination, infectious pathogens are detected in about 20% of patient with acute pericarditis.1 Among the infectious agents enteroviruses are the most common, while bacterial pathogens such as Mycoplasma pneumoniae, Coxiela burnetii, Borrelia burgdorferi, Brucella species, or tuberculosis, are found much more rarely.2,3 However, many practitioners give up an extensive microbiological work-up, especially for viruses, generally because there is no specific antiviral therapy. Although relapsing pericarditis is usually considered idiopathic, probably most of them are autoimmune diseases.4 Infectious recurrent pericarditis may only seem of such a nature as relapse occurs due to interruption of anti-infectious therapy.1,4C. burnetii is capable of causing a wide spectrum of acute and chronic infections. A chronic infection is considered to be confirmed by phase I IgG antibody titre, generally determined by the indirect fluorescence antibody (IFA) test. A chronic infection requires antibiotic administration for 18-24 months and in some cases for an indefinite period, and doxycycline combined with rifampicin, or ciprofloxacin, or hydroxychloroquine is a recommended treatment.5 We present a rare case of chronic C. burnetii infection with a clinical feature of recurrent pericarditis. 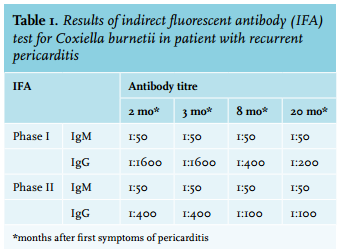
CASE REPORT
A 76-year-old male patient was hospitalised following three weeks of progressive fatigue, with a fever up to 37.8 °C, chest tightness and dyspnoea on physical effort. The patient had chronic atrial fibrillation, but he felt well and was not taking any medication. There were no data about other chronic diseases, and the patient had not undergone any surgical procedures such as prosthetic heart valve or vascular graft placement. Physical findings on admission were unremarkable. Electrocardiography showed atrial fibrillation with a ventricular response of 80 beats/min. Thoracic multi-slice computed tomography and transthoracic echocardiography (TTE) showed a circumscribed 3-mm pericardial effusion ahead of the right ventricle, a partially organised 8-mm effusion behind the posterior wall of the left ventricle and thickening of parietal pericardium; the valvular apparatus was found to be normal. The erythrocyte sedimentation rate (ESR) was 72 mm/1 hour, C-reactive protein (CRP) 85 mg/l, leukocytes 4.6 x 109/l (neutrophils 72%); red blood cells, platelets, serum biochemistry findings, tumour markers (CEA, CA15.3, CA19.9) and thyroid hormones were within the normal limits. When selecting empiric treatment, idiopathic pericarditis, as well as infectious pericarditis such as that caused by Mycoplasma pneumoniae, were taken into consideration. Therapy with colchicine 275 mg three times a day for three weeks plus doxycycline 100 mg twice daily for two weeks was introduced. The patient became afebrile with subsequent reduction of symptoms, normalisation of laboratory findings, and minimal pericardial effusion at discharge. Two weeks after treatment discontinuation, the symptoms of pericarditis reappeared, and he turned febrile with a temperature up to 39 °C. Physical findings were unremarkable again, there was no heart murmur, and peripheral arterial pulsations were normal. TTE showed 4 mm of pericardial effusion in diastole, located behind the posterior wall of the left ventricle; the valvular apparatus was normal, without haemodynamic impairment, and no masses or floating formations were found. Chest X-ray findings were normal. ESR was 76 mm/1 hour, CRP 158 mg/l, and leukocytes 7.3 x 109/l (neutrophils 81%), and Mantoux test with two purified protein derivative (units produced induration of 6 mm in diameter. Antinuclear antibodies, blood cultures, as well as serology for brucellosis, Mycoplasma pneumoniae, and Chlamydia pneumoniae were negative. Serological testing for C. burnetii was done at the Department of Clinical Microbiology, University Hospital Split, using the Q Fever Dual-Spot IFA (Focus Diagnostics, Cypress, California, USA), and its result indicated chronic infection (table 1). Subsequently, the patient recalled that he occasionally visited his relatives engaged in sheep wool processing, but he could not recall any febrile illness in the recent past that could be associated with C. burnetii infection. Doxycycline alone, without anti-inflammatory therapy, was re-introduced. The patient became afebrile within seven days, his subjective discomfort gradually subsided, and the laboratory findings normalised. Due to prolonged doxycycline-induced diarrhoea he refused addition of hydroxychloroquine, and finally discontinued doxycycline having completed nine months of therapy. After three months of treatment, TTE showed normal findings and he was completely free of symptoms. Two years later, he was still free from pericarditis relapse, and phase I IgG titre showed an 8-fold drop.
DISCUSSION
Pericarditis is a rare manifestation of C. burnetii infection. Among 1383 patients with C. burnetii infection, Raoult et al. found that 1% had acute pericarditis.6 However, up to 3.5% of the cases of acute pericarditis diagnosed as idiopathic have been shown to be caused by acute C. burnetii infection.3,7 Recurrent pericarditis is most frequently idiopathic.2 However, some of these recurrent cases refer to the incessant type of pericarditis in which disease relapse occurs within six weeks of discontinuation of anti-inflammatory therapy.4 Reviewing the literature we only found three cases of chronic pericarditis briefly described by Raoult and al.6 Just as our patient, all three showed a feature of relapsing pericarditis with phase I IgG titres ≥ 1:800. Phase I IgG titre of 1:1600, as found in our patient, confirms chronic infection with a predictive value of > 95%.5,6C. burnetii infection is common in southern Europe, in particular among people living in rural areas.6,8 Therefore, serology for C. burnetii infection, preferably IFA, is advisable in the aetiological work-up of all pericarditis cases in countries with a high incidence of C. burnetii infection. Finally, in a case of prolonged and/or recurrent pericarditis, phase I IFA testing should be done in search of chronic C. burnetii infection. Such an approach could widen our knowledge about aetiology and optimise the therapeutic management of these types of pericarditis.
REFERENCES