KEYWORDS
Diverticulitis, coloenteric, fistula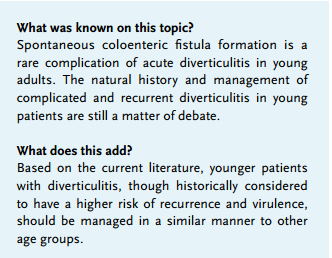
INTRODUCTION
Internal intestinal fistulae between the colon and small bowel can occur in postoperative, chronic infection or inflammatory states.1 Spontaneous fistulae are commonly found in Crohn’s disease and less commonly in complicated diverticulitis. Colovesical fistulas constitute the most common type of spontaneously occurring fistulas associated with diverticular disease2 while coloenteric fistulas are relatively uncommon.3
The natural history and the management of complicated and recurrent diverticulitis in young patients are still a matter of debate. Here we describe a case of a young patient with history of recurrent diverticulitis complicated by coloenteric fistula formation. We also review the natural history, outcome and management of acute diverticulitis in young adults.
CASE REPORT
A 38-year-old male patient presented with left lower quadrant abdominal pain, nausea, vomiting and chills for three days. He also reported a weight loss of 35 pounds over a six-month period. The patient’s past medical history was notable for schizophrenia, migraine headaches and two prior episodes of acute diverticulitis. His physical exam revealed an ill looking middle-aged male with abdominal tenderness and a palpable mass in the left lower quadrant. The rest of the physical examination was otherwise unremarkable.
His initial lab results showed a white blood cell count of 12.5 x 109/l, haemoglobin 10.24 mmol/l, and platelets 316 x 109/l. The rest of his lab work was negative (or normal) including liver function tests, kidney function tests, albumin, C-reactive protein, urine analysis and carcinoembryonic antigen. Computed tomography (CT) scan of the abdomen and pelvis with contrast showed diverticulosis of the colon, prominent inflammatory changes surrounding the lower descending colon and proximal sigmoid colon, and an ill-defined pelvic mass involving the sigmoid colon and ileum with a question of possible invasion into the bladder (figure 1). The patient was evaluated by a surgery team who recommended supportive treatment with a nothing by mouth status, intravenous fluids, intravenous antibiotics and a colonoscopy once the acute inflammation resolved to rule out malignancy.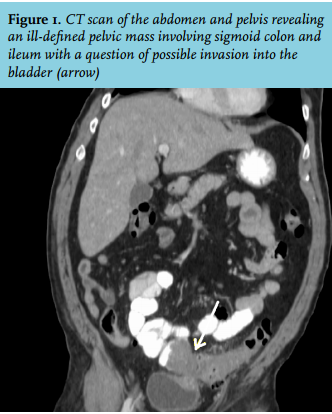
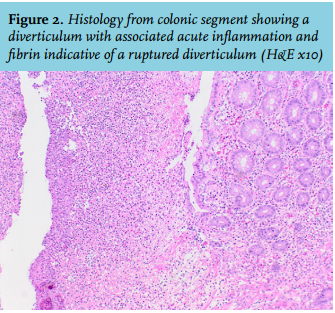
The C-reactive protein value was not repeated to evaluate resolution of the inflammation because it was normal on admission. Colonoscopy was performed on day 5 of admission after the patient’s white blood cell count normalised and his symptoms improved. Colonoscopy examination revealed extensive diverticulosis, an abrupt transition from colonic vascular mucosa to granular and glistening mucosa of what appeared to be small bowel at approximately 30 cm from the anal verge, consistent with a coloenteric fistula. A biopsy was taken which confirmed small bowel mucosa. No masses were identified in the colon. Cystoscopy did not reveal any evidence of fistula involving the urinary bladder and the patient was taken to the operating room where he underwent adhesiolysis, segmental left colectomy, small bowel resection, jejunojejunostomy and colo-rectal anastomosis. Surgical pathology confirmed multiple diverticulae with acute diverticulitis, abscess formation and acute serositis consistent with a ruptured diverticulum in the colonic segment (figure 2) with the small bowel segment showing evidence of a coloenteric fistula tract (figure 3). The patient did well postoperatively and made a full recovery.
DISCUSSION
Almost 25% of patients with acute diverticulitis develop complicated diverticulitis, defined as development of a perforation, phlegmon, abscess, stricture or fistula.4 Fistulas comprise approximately 2-4% of complicated diverticulitis. About 60% of these fistulas are colovesical, 30% are colovaginal and only 3% of these fistulae are reported as coloenteric.2 About 50% of patients with colovesical fistulas are diagnosed with diverticulosis after the fistula becomes clinically evident. Endoscopic evaluation of colovesical fistulae traditionally has a low yield, with a reported detection rate of less than 10%.5,6 However, evaluation of the remainder of the colon by colonoscopy is important to rule out concurrent disease processes including malignancy.7
In the United States, complicated disease at presentation is more common in African-American patients and in individuals who lack medical insurance (based on an analysis from the Nationwide Inpatient Sample).8
Diverticulitis in the young has been treated as a special subset due to previous reports of high virulence, higher recurrence and the need for more frequent surgery.9-12
However, several studies indicate that young age in itself is not a predictive factor of poor outcome in the management of first or recurrent episodes of acute diverticulitis.13-22
Guzzo and Hyman examined 762 patients admitted to their institution with sigmoid diverticulitis between 1990 and 2001, including 259 individuals younger than 50. The risk of requiring surgery during the first admission was comparable between older and younger patients. In addition, out of 196 younger patients who were treated medically at the time of their initial admission, only one (0.5%) presented with perforation during a median follow-up of 5.2 years.13 West et al. reported that diverticulitis in young patients at their institution did not appear to take a more aggressive course than the same disease in older patients.14 Similar conclusions were made by Ritz and colleagues when they assessed the clinical outcome of 1019 patients with acute diverticulitis presenting between 1998 and 2010.15 A recent study by Ünlü et al. also highlighted that younger age is neither associated with a more severe presentation of diverticulitis nor with a higher incidence in recurrence,16 which is in accordance with two other studies.17,18
In terms of management of acute and recurrent diverticulitis in young adults, a study performed by Nelson and colleagues proposed that young patients with uncomplicated disease findings as defined by CT criteria should be managed according to the same guidelines as those used for older populations.19 In a retrospective study performed by Faria et al. comparing the course of acute diverticulitis in younger and older patients after stratification of diverticulitis according to the Hinchey classification, the authors recommend that diverticulitis management should be based on the severity of the disease and not on the age of the patient.20 Furthermore, a study by Kotzampassakis et al. concluded that there was no difference in the rate of successful conservative treatment between patients with a first episode and those with recurrence in either age group.21 Finally, a recent meta-analysis performed by Katz and colleagues proposed that factors other than age should also be considered while choosing a therapeutic regimen for acute diverticulitis.22
Based on the available contemporary data, it appears that young age in itself is not a predictive factor of poor outcome in the management of first or recurrent episodes of acute diverticulitis. There does not seem to be sufficient justification to recommend elective surgery after one attack of sigmoid diverticulitis in younger patients and rather the disease should be treated similarly in both younger and older patients depending on its severity and inclination to recurrence.
CONCLUSION
Spontaneous fistulae from acute diverticulitis remain an uncommon complication. Prompt diagnosis and adequate antibiotic treatment remain the mainstays of the management of patients diagnosed with acute diverticulitis with surgery reserved for exceptional cases. However, recurrent episodes of diverticulitis, especially in non-compliant patients with suboptimal care, can lead to complications such as fistulae. Younger patients should be managed in a similar manner as other age groups based on the current literature.
DISCLOSURES
The authors declare no conflict of interests. No funding or financial support was received.
REFERENCES