KEYWORDS
Good’s syndrome, secretory diarrhoea, thymoma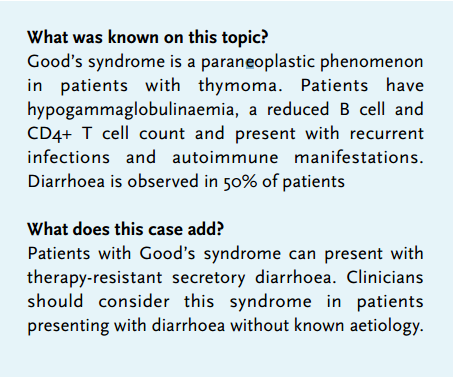
CASE REPORT
A 74-year-old Caucasian woman was referred to our centre because of therapy-resistant secretory diarrhoea for six weeks, resulting in severe weight loss of 15 kilograms (27% of her total body weight). Her medical history included oral lichen planus and atypical nodular lesions on her legs, diagnosed as keratoacanthoma. Four weeks after onset of diarrhoea, a colonoscopy was performed which revealed active colitis and nonspecific inflammation on pathological examination. On macroscopic examination during colonoscopy and microscopic examination the colitis was regarded as not specific for cytomegalovirus. Corticosteroids and mesalazine were started. However, after a few days she was admitted to the intensive care because of renal impairment and severe metabolic acidosis due to excessive gastrointestinal fluid and bicarbonate loss. Repeated blood and faecal cultures, including Salmonella, Shigella, Yersinia, Campylobacter and Clostridium, remained negative. The patient was tested for HIV and found negative.
A paraneoplastic disease was suspected as the aetiology of the secretory diarrhoea. Octreotide was started to control fluid and electrolyte loss. Computed tomography (CT) scanning was performed in search of a neuroblastic or neuroendocrine tumour or thymoma. An anterior mediastinal mass was detected on chest X-ray and subsequent fluorodeoxyglucose (FDG) positron emission tomography (PET) with low-dose CT (FDG-PET/CT) scanning showed some uptake in this anterior mediastinal mass, without uptake in mediastinal lymph nodes or distant localisation. Figure 1 shows the chest X-rays and an image of the CT scan with the anterior mediastinal mass. The findings were consistent with thymoma.
At that time the patient developed leukopenia and lymphocytopenia. The immunoglobulins were very low: IgA < 0.07 g/l (0.7-4.0 g/l) and IgM < 0.04 g/l (0.4-2.3 g/l). IgG was normal, but IgG subclass 4 was decreased (< 0.07 g/l (0.08-1.4 g/l)). The paraneoplastic antibody vasoactive intestinal polypeptide was negative.
The combination of secretory diarrhoea, an anterior mediastinal mass and hypogammaglobulinaemia were suggestive for Good’s syndrome.
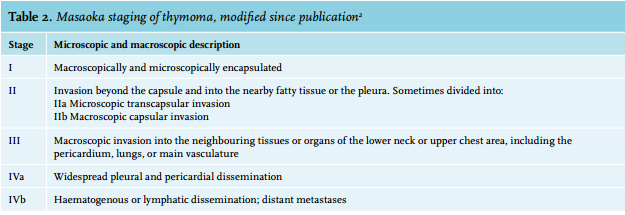
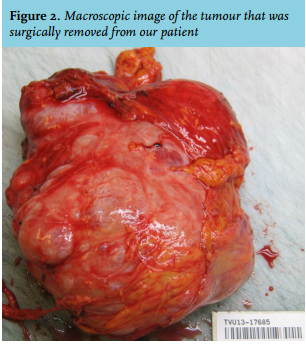
Thymectomy via sternotomy was scheduled and performed uneventfully. Pathological examination of the resected specimen confirmed the suspected diagnosis: in this case type A thymoma of 13.8 cm in diameter with clear surgical margins according to the WHO classification of thymomas1 (table 1). Figure 2 shows a macrophoto of the thymoma with intact encapsulation. Type A thymoma is a medullary subtype composed of bland spindle cells and few lymphocytes. The tumour was encapsulated, both on macroscopic and microscopic examination. Therefore, the patient was classed as Masaoka stage I thymoma2 (table 2). After surgery, her condition improved and the diarrhoea resolved. During follow-up, diarrhoea did not recur, neither did patient suffer from any infections. 
DISCUSSION
Good’s syndrome is a paraneoplastic phenomenon associated with thymoma, which was first described by Robert Good in 1954.3 Thymoma is a rare epithelial neoplasm originating from the thymus gland. This organ in the anterior mediastinum is present at birth and normally involutes at older age. Patients with thymoma may complain of symptoms secondary to the location of the anterior mass. These symptoms include hoarseness, dysphagia, dyspnoea, cough and chest pain. Histologically, thymomas are classified based on the shape of the epithelial cells. The prognosis for Masaoka stage I is excellent.2
Thymoma is best known for its association with myasthenia gravis, but it is also associated with other paraneoplastic syndromes. Patients with Good’s syndrome typically have hypogammaglobulinaemia and a reduced B cell and CD4+ T cell count. The clinical presentation is usually determined by the underlying immunodeficiency. This affects both humoral and cellular components.4
The pathogenesis of Good’s syndrome is unclear but the haematological deficiencies suggest an underlying bone marrow disorder. The majority of patients (83%) present with recurrent infections, followed by autoimmune manifestations (59%) such as oral lichen.4,5 In almost 50% of patients, diarrhoea is the presenting symptom of Good’s syndrome.4-6 Thus far, the underlying mechanism of secretory diarrhoea associated with Good’s syndrome is unclear. However, several mechanisms are postulated. Diarrhoea might be related to an infectious aetiology, as in some patients a pathogen is found such as Salmonella, cytomegalovirus, Campylobacter and Giardia lamblia, or bacterial overgrowth is detected.7 In our patient, no infectious pathogen was found, neither in faecal nor blood cultures.
Another aetiology of diarrhoea associated with Good’s syndrome that is proposed is described as an autoimmune enteropathy with watery diarrhoea and malabsorption, due to mucosal lesions and villous atrophy as autoantibodies against enterocytes can be found in some patients.7,8 The mechanism of autoimmunity is not completely understood, but it might be associated with disordered thymic epithelial function.8 In healthy individuals, the thymus is involved in the processing and maturation of T-lymphocytes that are released into the circulation upon maturation. Thymomas can disrupt this function.8
Furthermore, multi-organ involvement is also described in the literature.8,9 Patients can present with chronic diarrhoea, skin eruptions and abnormal liver enzymes. Histopathological findings of bowel mucosa are similar to that seen with graft-versus-host disease.
Good’s syndrome is treated by thymectomy, and infection prevention by giving gamma globulins and prophylactic antibiotics. Despite this treatment, the majority of patients succumb to the consequences of immunodeficiency and autoimmune diseases, with a ten-year survival of only 33%.8
In our patient, the diarrhoea almost immediately improved after surgery. This suggests an autoimmune pathogenesis with disrupted thymic function. However, symptoms can persist or even arise years after thymectomy.6
Diarrhoea can be used as a follow-up marker for our patient or for patients who presented with this symptom. If the diarrhoea recurs, one should be aware that the tumour is back. This also applies to recurrent infections.
Finding the aetiology of therapy-resistant diarrhoea can be challenging when the most common causes are excluded and a patient remains therapy resistant. Imaging of the thorax in a patient with unexplained diarrhoea may lead to finding relatively rare paraneoplastic syndromes such as Good’s syndrome.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES