KEYWORDS
HRQOL, nursing home, rehabilitation, mortality, aged
INTRODUCTION
Comorbidities, depression, cognitive impairment and other geriatric problems are highly prevalent in old age and can greatly impact health-related quality of life (HRQOL).1-6 As a consequence, HRQOL is generally low in nursing home residents.2-4,7-9 Nursing homes in the Netherlands provide care and long-stay services for elderly patients with chronic mental or physical diseases, and the majority also provide rehabilitation services. Measuring HRQOL in nursing home patients could lead to an increased understanding of factors that negatively impact HRQOL, ultimately aiming to improve the HRQOL of this patient group, characterised by an overall very low HRQOL.
The evaluation of HRQOL in indiviidual patients can be used to measure disease-related distress and overall perception of health. Next to the evaluation of HRQOL as a separate outcome measure, HRQOL also has prognostic value in non-nursing home settings. Furthermore, a lower HRQOL has been associated with increased mortality risk in non-nursing home settings, also in elderly patients. Besides, HRQOL is also used to evaluate therapeutic interventions. Therefore, HRQOL could have a variety of implications in decision-making processes regarding patients and medical interventions.
Increased understanding of HRQOL in nursing home patients could improve the HRQOL and outcome of these patients. As mortality risk is already very high in old age, other clinical outcomes, besides HRQOL itself, such as successful rehabilitation, may be more relevant. Several studies have reported a relationship between HRQOL and rehabilitation in, for example, stroke patients.10,11 Low HRQOL corresponds to substantial limitations in physical, emotional and social well-being due to a medical condition or its treatment.12 These aspects of HRQOL can negatively influence successful rehabilitation. The associations between HRQOL and rehabilitation may be bidirectional: on the one hand successful rehabilitation itself can improve HRQOL13-15 and on the other hand a higher HRQOL may improve motivation and increase the chance of successful rehabilitation.
To our knowledge, there are no studies that have investigated the relationship between HRQOL and rehabilitation in a nursing home. Only one study investigated the relationship between HRQOL and mortality in a nursing home setting.16
Furthermore, no studies have reported whether measuring HRQOL had a discriminatory value, using for example the Harrell’s C to assess the predictive capability of HRQOL in a nursing home population. The continuous growth of the elderly population in combination with the severely impaired HRQOL in our oldest old underlines the importance to gain more understanding of the implications of HRQOL in nursing home populations. The purpose of this study was to investigate the associations between HRQOL and two clinically relevant outcome measures, all-cause mortality and successful rehabilitation, in patients admitted to a nursing home.
MATERIALS AND METHODS
The study is reported according to the STROBE (Strengthening The Reporting of Observational Studies in Epidemiology) recommendations.17
Study sample
The design and details of this prospective observational cohort study have been described previously.18 Only patients from rehabilitation and somatic departments were included. Patients admitted to a somatic department receive prolonged or permanent care whereas patients in the rehabilitation department are admitted with the intention to rehabilitate and return home. Recruitment and all study procedures, for example administering the HRQOL questionnaire, for patients in the somatic department took place between September 2010 and December 2010. Timing of inclusion was different for each somatic patient. For patients in the rehabilitation department, recruitment and all study procedures took place between September 2010 and December 2011, mostly within the first weeks of admission
Patients admitted to the psychogeriatric department were excluded, because these patients are generally not able to complete HRQOL questionnaires.19 Other exclusion criteria were a life expectancy less than four weeks and an impending transfer to a hospice department.
Data collection
An elderly care physician collected all baseline data directly after inclusion. Baseline data included demographic characteristics, full medical histories (including cardiovascular disease (CVD), diabetes mellitus and hypertension), and medication use. Trained physicians or nurses administered the questionnaires at baseline. HRQOL was measured using the RAND-36 questionnaire.12,20 The RAND-36 is a generic instrument to measure aspects of health that are relevant to functional status and well-being.20,21 The RAND-36 consists of nine aspects of health status: physical functioning, role limitations due to physical problems (role functioningphysical), bodily pain, general health, vitality, social functioning, role limitations due to emotional problems (role functioning-emotional), mental health, and health change. Each dimension has a 100-point scale, where higher scores indicate better HRQOL. Of the nine scales two component summary scores can be calculated: a physical component summary (PCS) and a mental component summary (MCS). In 2015, vital status and cause of death were retrieved from the records maintained by the nursing home and general practitioners.
Clinical outcome measures
All-cause mortality and successful rehabilitation were the primary endpoints. Successful rehabilitation was defined as either discharge to the patient’s own home or an adapted home for the elderly, where they were self-reliant. Successful rehabilitation was investigated in the subgroup of patients admitted to the rehabilitation department.
Statistical analyses
Continuous variables are presented as mean with the standard deviation for normally distributed variables, or as median with an interquartile range (IQR) for non-normally distributed variables. Cox proportional hazard modelling was used to investigate the relationship between HRQOL and: 1) all-cause mortality and 2) successful rehabilitation, with and without adjustment for the following confounders: age, gender, smoking, body mass index, a history of cardiovascular, or pulmonary disease, hypertension, psychiatric disease, length of stay before study inclusion, and the number of medications they were using. Collinearity was tested between each of the RAND-36 dimensions and the confounders. All hazard ratios refer to a ten-point higher score on the RAND-36 dimensions. In case of significant associations in the Cox regression models, risk prediction capabilities were assessed with Harrell’s C statistics and the proportion of explained variance (R2 ).22,23 The Schoenfeld residual plots were inspected for each predictor variable to check the assumption of proportional hazards; all assumptions were met unless stated otherwise. A two-sided p < 0.05 was considered significant. All statistical analyses were performed using SPSS software version 22 (IBM, Armonk, New York, USA) and STATA (version 13; StataCorp, College Station, Texas, USA).
Ethical approval and clinical trial registration
Before starting the study, the Central Committee of Research Involving Human Subjects (CCMO) in the Netherlands was contacted. The CCMO agreed that with the current design, no formal approval of an accredited medical ethics committee was needed. According to Dutch guidelines this research does not fall under the scope of the Medical Research Involving Human Subjects Act. This study was performed in accordance with the Declaration of Helsinki, the treating physicians and nurses obtained written informed consent from all patients and data were analysed anonymously. The study was registered on ClinicalTrials.gov (NCT01362751).
RESULTS
A total of 184 patients were included in this cohort. HRQOL data were completed for 159 (86%) patients. From the 159 included patients, 123 patients were admitted to the rehabilitation department and 36 to the somatic department. Baseline characteristics of the total study population are presented in table 1. The median age (IQR) was 79.2 (75.2-85.9) years. Median PCS and MCS (IQR) scores were 44 (34-57) and 59 (48-74), respectively.
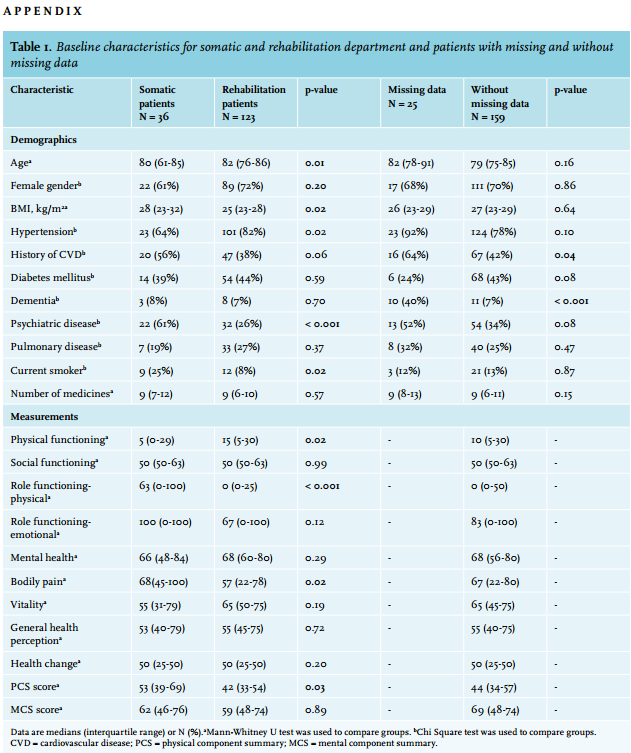
Patients in the rehabilitation department were older, had a lower BMI, hypertension was seen more frequently, and psychiatric disease was seen less often compared with patients in the somatic department (Appendix table 1). No difference in mortality hazard was observed between the rehabilitation department and the somatic department (hazard ratio (HR) 0.90 (95% confidence interval (CI) 0.66-1.21). Patients with missing data had a higher history of dementia and CVD compared with patients without missing data (Appendix table 1). Missing data were not significantly associated with mortality or successful rehabilitation, HR 0.89 (95% CI 0.47-1.71) and HR 1.41 (95%CI 0.47-4.23), respectively. 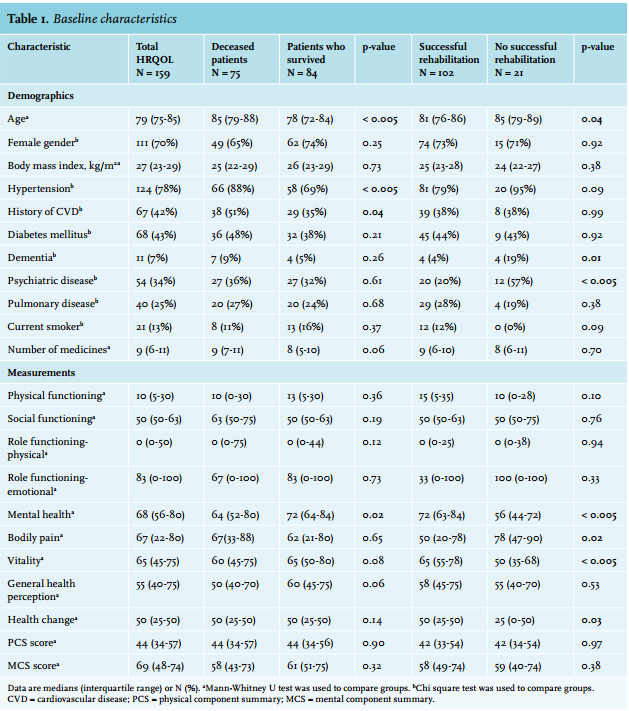
HRQOL and mortality
During a median follow-up period of 3.4 years, 75 (47%) patients had died. Three out of nine health dimensions were independently associated with all-cause mortality (after adjusting for confounders). The health dimensions vitality and mental health were inversely associated with mortality: HR 0.88 (95% CI 0.77-0.99) and HR 0.86 (95% CI 0.75-0.98), respectively. The dimension role functioning-physical was positively associated with mortality: HR 1.08 (95% CI 1.02-1.15). PCS and MCS component scores were not significantly associated with all-cause mortality. In model 2, age was the only covariate besides the above-mentioned three health dimensions, which was significantly related to mortality (HR 1.08 (95% CI 1.04-1.12)). The results of the Cox regression analyses are presented in table 2.
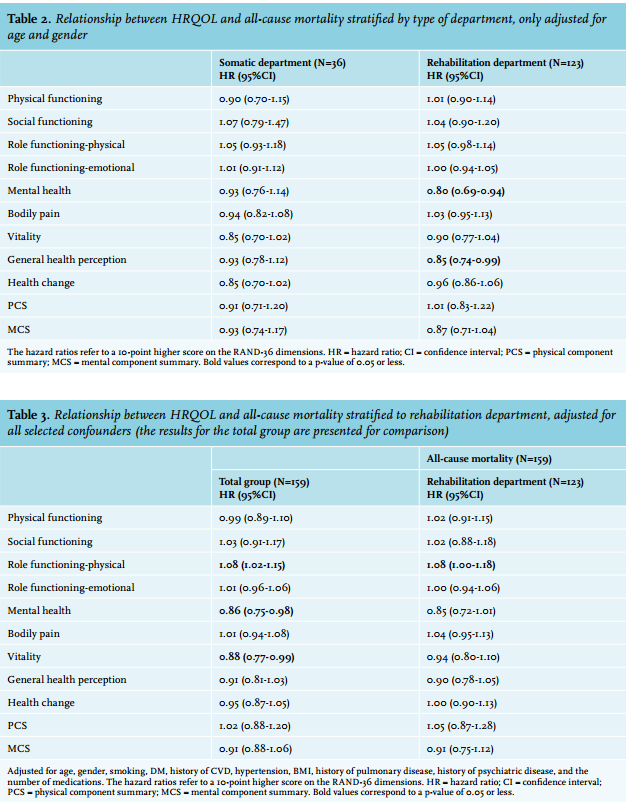
Post-hoc analyses were performed according to type of department. Because of the small number of somatic long-term patients (n=36), we first adjusted for age and gender in both groups (Appendix table 2). The analyses with the fully adjusted model were only performed for the rehabilitation group (Appendix table 3). In additional analyses, stratified according to type of department, no significant associations were seen between HRQOL and mortality within the group of somatic patients. Within the rehabilitation group significant relations with mortality were observed for the dimensions mental health and general health perception: HR 0.80 (95% CI 0.69-0.94) and HR 0.85 (95% CI 0.74-0.99), respectively. After adjustment for all selected confounders, a significant relationship in the rehabilitation group was only seen between the dimension role functioning-physical and mortality (HR 1.08 (95% CI 1.00-1.18)).
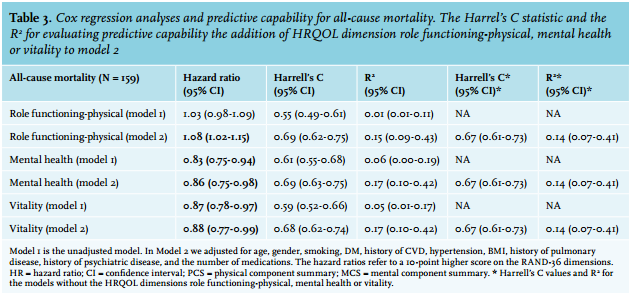
The results of the analyses regarding the risk prediction capabilities are presented in table 3. The Harrell’s C values for the adjusted model of the dimensions role functioningphysical, mental health and vitality were 0.69 (95% CI 0.62-0.75), 0.69 (95% CI 0.63-0.75) and 0.68 (95% CI 0.62-0.74), respectively. The Harrell’s C values and the R2 were ≤ 0.02 and ≤ 0.03 higher in the models with the HRQOL dimensions role functioning-physical, mental health or vitality compared with the models without these three dimensions.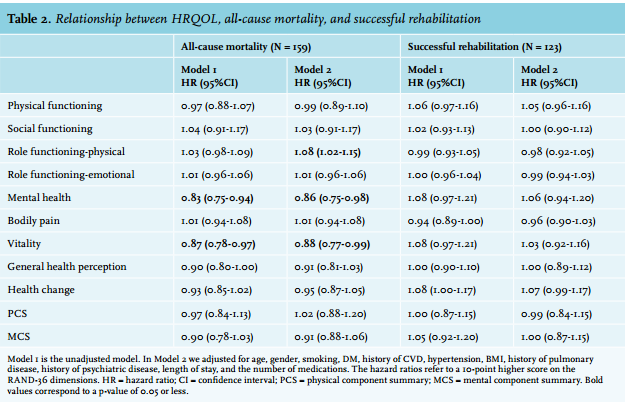
HRQOL and successful rehabilitation
Data on HRQOL were missing for 5 (4%) out of 128 patients admitted to the rehabilitation department. During a median follow-up period of 36 days (IQR 7-88), 102 patients were successfully rehabilitated; 90 patients were discharged to their own home and 12 were discharged to an adapted home for the elderly. Patients who were successfully rehabilitated had higher scores on the subscales mental health, vitality and health change, while they scored lower on the subscale bodily pain. None of the health dimensions or summary scales were significantly associated to successful rehabilitation in the regression analyses (table 2).
DISCUSSION
HRQOL was significantly associated with mortality for three dimensions, but partly in opposite directions. We observed no independent association between HRQOL and successful rehabilitation.
HRQOL and mortality
During a median follow-up period of 3.4 years, 75 (47%) patients died. There is great variation in mortality rates in nursing home studies.16,24,25 Because nursing homes could provide care for patients with chronic mental or physical diseases or provide rehabilitation services or combined, mortality rates strongly depend on the type of nursing home. Taking this all together, it is difficult to make a reliable comparison of the mortality rates between the current and previous studies.
Higher scores on the dimensions vitality and mental health were related to a lower mortality risk, whereas a higher score on the dimension role functioning-physical was related to a higher mortality risk. The Harrell’s C values and the R2 were ≤ 0.02 and ≤ 0.03 higher in the adjusted models with the dimensions role functioning-physical, mental health or vitality compared with the models without these dimensions.
The score on the role functioning-physical dimension expresses the problems in daily life caused by a physical condition. The positive association with mortality implies that experiencing fewer problems in daily life was associated with an increased mortality risk, which is counterintuitive and has not been previously reported. A possible explanation could be that these frail patients are accustomed to living with substantial limitations in functioning, and therefore scored low on this dimension. In addition, and probably even more relevant, this scale may be inappropriate for nursing home residents as the scale is composed of four individual questions which relate to work or daily activities. Finally, the results could be due to a type 1 error.
The mental health and vitality dimensions were inversely associated with mortality, which was as we had expected and confirmatory to results from prior studies in different populations.26-30 The mental health dimension is related to depression and anxiety and the vitality scale is related to fatigue and apathy. In a previous study in a nursing home setting, only physical functioning was significantly related to mortality.16 Despite the fact it was a nursing home population, the study population was very different compared with the present study. Mainly long-term residents were included and a high percentage (26%) of these residents had cancer, which may have resulted in different complaints and limitations, resulting in different HRQOL scores, but also in a different mortality risk.
Within the rehabilitation department, the dimension role functioning-physical was positively related to mortality. Within the somatic department no relation with HRQOL and mortality was found. This difference in results between the somatic and rehabilitation department could be explained by the fact that patients rehabilitating in a nursing home are potentially physically more frail after a recent acute hospital admission. Patients in the somatic department are chronic patients and used to their physical status. Furthermore, patients admitted to the rehabilitation department were older compared with patients on the somatic ward. Because of the sample size, we cannot exclude that the stratified results concerning the somatic group were subject to a type 2 error.
Another study in community-dwelling elderly described a significant relationship between all subscales and mortality.31 In comparison with the present study, these community-dwelling elderly were not admitted patients but were selected by a demographic registration system, which probably explains the difference in HRQOL scores and may explain the other relationship with mortality.
In the present study the physical and mental component summary scores were not significantly related to all-cause mortality. This can be explained by the fact that the component summary scores are calculated from nine health dimensions, while only three health dimensions were significantly related to mortality. Besides, this could also be due to the sample size or the duration of follow-up. A previous study in community-dwelling elderly patients with type 2 diabetes showed that MCS was only associated with mortality after an extended and long-term follow-up period.29 If HRQOL is indeed only related to mortality after a long follow-up period, using HRQOL for these prognostic capabilities will be irrelevant as a long follow-up is not feasible in an old and frail population.
Although our study showed that the dimensions role functioning-physical, vitality and mental health were an independent risk factor for mortality, based on a minimal increase in Harrell’s C values when adding role functioning-physical, vitality or mental health to the adjusted models, one may conclude that the additional value of these dimensions in mortality prediction is apparently very limited. It is important to realise that this study group is a group of frail patients with much comorbidity. Even in the fully adjusted models, the C value was lower than 0.70, indicating the poor predictive capability of the overall model.
HRQOL and successful rehabilitation
The results of the present study showed no significant association between HRQOL and successful rehabilitation. We hypothesised that higher HRQOL scores would be associated with successful rehabilitation. Due to better physical, emotional and social well-being, rehabilitation targets would be achieved sooner. Assessing changes in HRQOL could be used to measure improvements in relation to the rehabilitation process.
Although HRQOL was not significantly associated with successful rehabilitation, there was an inverse relationship between a history of psychiatric disease and successful rehabilitation (HR 0.41 [95% CI 0.24-0.69]). In previous studies the relationship between depressive symptoms and functional recovery has been described in post-stroke patients.32,33 Depression has a negative effect on recovery in functional status and treatment of depressive symptoms leads to enhanced rehabilitation.
Several previous studies showed improvements in HRQOL after different types of rehabilitation in diverse patient groups (stroke, COPD, cardiac problems, cancer),11,14,34,35 but the aims of these studies differed from the aim of the present study. In the present study we aimed to investigate the exact opposite, whether HRQOL could influence the rate of successful rehabilitation. To the best of our knowledge, there are no validation studies regarding the use of the RAND-36 in rehabilitation patients. Concerning its use in a nursing home population, a validation study has been performed.19 It can be questioned if the SF-36 or RAND-36 is a valid instrument in a nursing home population. Possibly, the SF-36 or RAND-36 could only be used for subgroups of rehabilitation patients, such as those with a higher cognitive and physical functioning.
Although we cannot exclude the possibility that rehabilitation itself may have positive consequences for HRQOL, the current study shows that baseline HRQOL is not related to an increased chance of successful rehabilitation.
Strengths and limitations
The main strengths of this study were the prospective design, the possibility to take into account the number of variables adjusted for in the multivariate model, and the representative group of nursing home patients.
Representativeness was based on the fact that 86% of all admitted somatic or rehabilitation patients during the study period participated in the present study. In addition, admission to a Dutch nursing home requires approval of a central indication committee and finally, the nursing home facility in the present study was a general nursing home, with somatic, psychogeriatric and rehabilitation departments, comparable with other Dutch nursing homes. There were also limitations. Firstly, due to the observational design it was not possible to establish a causal relation between HRQOL and mortality. Secondly, the RAND-36 questionnaires were not completed in 14% of the sample and this could have led to an uncertainty in the effect estimate. On the other hand, missing data were not significantly associated with mortality or successful rehabilitation: HR 0.89 (95% CI 0.47-1.71) and HR 1.41 (95% CI 0.47-4.23), respectively. The inability to complete questionnaires is a frequently observed problem in geriatric studies and indicative for severe morbidity. However, previous studies that investigated the RAND-36 had a lower response rate compared with present study.29,30,36
Thirdly, the adequacy of using the RAND-36 questionnaire within a nursing home population has been questioned in different studies.4,19 An important issue is that the RAND-36 entails several potentially inappropriate questions for this population.4,19 Due to the high heterogeneity in the nursing home population in general, the use of the RAND-36 could be more suitable for subgroups of rehabilitation patients, such as those with a higher cognitive and physical functioning.19
Fourthly, we did not investigate changes in HRQOL. A change in HRQOL could possibly have predicted mortality more accurately.37 Fifthly, successful rehabilitation was defined as discharge to home or a home for the elderly, where they remained self-reliant. As a consequence, patients with a worse outcome after rehabilitation but with a highly adapted home environment (e.g. stair lift, homecare, meal service) might have been discharged sooner. Finally, our study sample is rather small and therefore our results may be a matter of coincidence.
Confirmation of our results in other studies is necessary, preferably performed with HRQOL at several moments during rehabilitation.
CONCLUSIONS
HRQOL was significantly associated with mortality for three dimensions, but partly in opposite directions. The additional value of HRQOL in mortality prediction is very limited. There were no independent associations between HRQOL and successful rehabilitation. The evaluation of HRQOL is important as a goal on its own; however, this study did not provide evidence for an association between HRQOL and successful rehabilitation within a nursing home population.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
REFERENCES