KEYWORDS
Lipid rescue, intoxication, hydroxychloroquine
INTRODUCTION
Hydroxychloroquine is well known for its antimalarial, antirheumatic and antilupus properties.
Hydroxychloroquine poisoning is a rare but often fatal intoxication due to mainly cardiovascular toxicity. We present two patients who survived severe intoxication with hydroxychloroquine, in a dose that was previously considered to be lethal, using the usual supportive care and intravenous lipid emulsion.
CASE REPORT
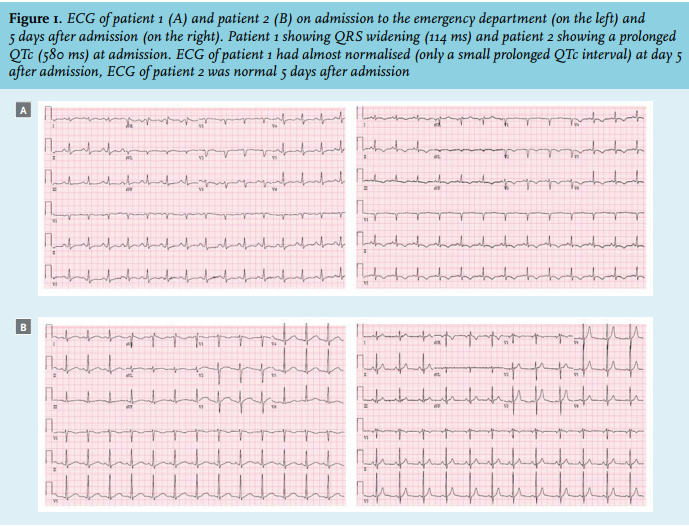
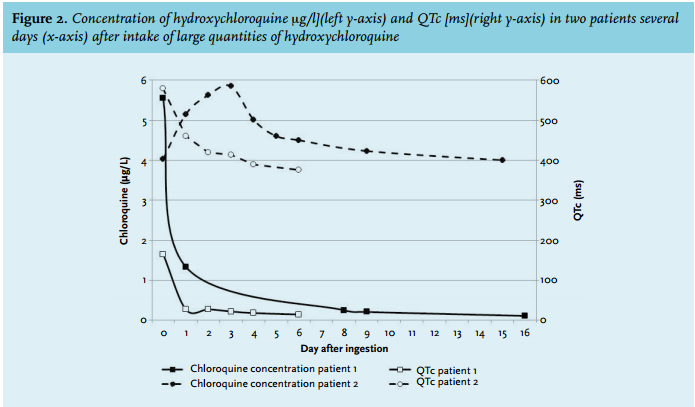
The first case involves a 25-year-old female who ingested about 17.5 grams of hydroxychloroquine and about 550 mg diazepam in a suicide attempt, approximately one hour before presentation. An ECG showed QRS widening (figure 1). Abnormal lab results included a hypokalaemia of 2.7 mmol/l (table 1). After an initially agitated state, she became unconscious, and developed hypotension, vomiting and eventually apnoea. The patient was intubated and intravenous access was established to administer norepinephrine, which was titrated to aim for a mean arterial blood pressure above 65 mmHg. Diazepam was given in a dose of 2 mg/kg/24 hours and this therapy was continued during the following eight days. Intravenous lipid emulsion 20% was started in a bolus of 1.5 ml/kg (100 ml) followed by continuous infusion of 0.25 ml/kg/min (400 ml) for 30 minutes, in an attempt to decrease the uptake of the lipophilic hydroxychloroquine. To treat the decreased ventricular conduction, 100 ml of sodium bicarbonate 8.4% was also administered. A bolus of potassium chloride (40 mmol) was given to supplement the hypokalaemia. After these interventions, haemodynamic stability was established within a few hours. Retrospectively, hydroxychloroquine serum concentration measured using liquid chromatographytandem mass spectrometry1 at admission was 5.5 µg/l. The hydroxychloroquine levels were measured several times in the next few days, showing a slow decline over time, which can be explained by the large volume of distribution (figure 2). Two days after admission, the ECG showed a prolonged QTc interval (figure 2), and serum cardiac enzymes were elevated (table 1). Both normalised within a few days. Transoesophageal echocardiography showed an overall decreased function, confirming cardiomyopathy. The potassium levels remained stable throughout admission, and a cautious approach was taken towards supplementation of potassium. Due to pleural effusion and sedation, the patient was intubated for eight days. Two days later she was transferred to the psychiatric department for further treatment of her suicidal symptoms and borderline behaviour. The patient recovered without sequelae.
The second case concerned a 25-year-old male who ingested about 5 grams of hydroxychloroquine, 10 mg codeine and 10 mg domperidone. On presentation to the emergency department, two hours after intake, his symptoms consisted of vomiting, a QTc of 580 ms (figure 1) and a hypokalaemia of 2.7 mmol/l (table 1). Knowing the positive outcome of the first case, this patient was also treated with the same dose of intravenous lipid emulsion, diazepam 2 mg/kg/24 hours, a restrictive policy towards supplementation of potassium and alkalisation of the blood using 100 ml of sodium bicarbonate 8.4%. The patient remained haemodynamically stable without signs of cardiomyopathy other than QTc prolongation. Therefore, vasopressor agents were not required. In the following days, the hydroxychloroquine levels and QTc gradually declined (figure 2). The patient recovered without sequelae.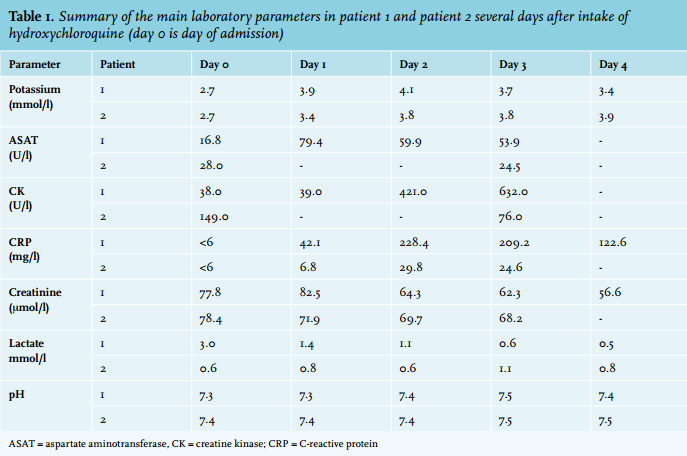
DISCUSSION
Hydroxychloroquine poisoning is a rare but often fatal intoxication. Since 2012 several newspapers in the Netherlands and Belgium heeded the unlimited availability of hydroxychloroquine as a suicide pill. The fatal dose of hydroxychloroquine in humans has not been established. Death has been reported after intake of 5 grams, although survival after more than 20 gram has also been reported.2 In both presented independent cases, the hydroxychloroquine was ordered via an Internet Pharmacy in order to attempt suicide. Although the exact number of tablets taken cannot be ascertained, the measured blood levels suggest the intake of a significant number of tablets.
Hydroxychloroquine is rapidly absorbed, with peak concentrations within one to two hours after intake. It has a large volume of distribution and a long elimination half-life.3 Most deaths occur within three hours after intake, which is attributed to the transiently high blood concentrations of hydroxychloroquine due to almost complete and rapid absorption.4 Therefore, early treatment is essential for prevention of complications, even in the absence of symptoms.5 In the first case, treatment was initiated within one hour after intake of hydroxychloroquine. In the second case treatment was started two hours after intake. It seems that this early treatment was necessary to prevent a fatal outcome.
After absorption, the blood concentration decreases exponentially due to a high volume of distribution of 200 l/kg. Therefore, toxic symptoms will rarely last for longer than 24 hours even though the terminal elimination half-life is prolonged, approximately 45-60 days and even longer for its active metabolites.6,7 Whole blood concentrations of hydroxychloroquine are known to be about 4-8 times higher than serum concentrations.6,8 Blood concentrations of 2.5 µg/l and above are considered to be lethal.5,7 Due to the high volume of distribution, haemodialysis and haemoperfusion is not effective in hydroxychloroquine intoxication.4,9,10
The toxicity of hydroxychloroquine is primarily associated with cardiovascular complications.11 Hydroxychloroquine has sodium channel blocking properties and therefore, acting as a class Ia anti-arrhythmic drug, will slow down ventricular conduction resulting in ventricular arrhythmias. Cardiovascular collapse mainly occurs because of a negative inotropic effect, but peripheral vasodilation leading to hypotension and collapse also occurs.3 Hypokalaemia, due to increased intracellular distribution of potassium, may worsen the cardiac effects of hydroxychloroquine.12 Other symptoms that might occur in hydroxychloroquine overdose are respiratory arrest, convulsions, coma and vomiting.13 In our patients, all symptoms of hydroxychloroquine overdose were present, of which the cardiac symptoms were the most disturbing. The main focus of treatment lies in preventing haemodynamic complications. Currently, effective treatment to improve outcome of severe intoxication with hydroxychloroquine consists of the use of epinephrine, diazepam and mechanical ventilation.5,13 In case of acute respiratory distress syndrome or refractory circulatory shock, treatment with extracorporeal membrane oxygenation could be considered.10
The use of (nor)epinephrine is common practice in the treatment of hydroxychloroquine intoxications. It reverses the cardiotoxicity of hydroxychloroquine by vasoconstriction and reduces the intraventricular conduction time.6,14 Furthermore, the conduction disorder was treated through alkalisation of the blood with sodium bicarbonate, which is also known to be effective in treating QRS widening caused by quinidine-like substances.3
Several reports suggest that diazepam has an antiarrhythmic effect in hydroxychloroquine poisoning, although the mechanism behind this remains unclear. Possibly, this effect is related to both decreasing the sympathomimetic output in the central nervous system as well as stabilising the membrane of cardiac muscle by binding to specific receptors.15,16 The concomitant intake of diazepam in the first patient could have prevented her from developing severe cardiotoxicity. However, in patients with acute intoxication of 2 or more but less than 4 grams, diazepam did not appear to reverse the hydroxychloroquineinduced membrane-stabilising effect.17
Most patients develop hypokalaemia due to increased intracellular distribution of potassium, which seems to have two opposite effects. A hypokalaemia may worsen pro-arrhythmic effects, but could also have a protective quality due to a compensatory mechanism tending to restore membrane excitability and inotropism by relative inhibition of the Na+/K+-ATPase pumps.12 Since hypokalaemia is not explained by depletion, correction of hypokalaemia should not be done aggressively, especially in the early hours.12
Intravenous lipid emulsion has been used successfully in systemic anaesthetic toxicity and in poisoning with several other lipophilic drugs.18 The use of intravenous lipid emulsion is described in our hospital protocol in case of local anaesthetic toxicity. However, because of previous, sometimes fatal, intoxications with other lipophilic compounds (e.g. calcium channel blockers and beta-blockers) intravenous lipid emulsion is usually advised and used in case of intoxications with these compounds. Intravenous lipid emulsion seems to be a safe therapy with hardly any side effects18 and therefore it was used as treatment option in these two cases. The mechanism of action of intravenous lipid emulsion is poorly understood but it is believed to primarily prevent lipophilic substances from distributing to target tissues. Hydroxychloroquine is a highly lipophilic substance with a lipid/aqueous partition coefficient (log P) of 4.3 comparable with that of local anaesthetics, which makes intravenous lipid emulsion a possible effective treatment.19 However, the evidence for the use of intravenous lipid emulsion for hydroxychloroquine toxicity is limited and only a few case reports have been published, with no positive outcomes so far.20,21 In this case report, the immediate use of intravenous lipid emulsion, within one to two hours after intake of hydroxychloroquine, whether or not combined with diazepam, could have played a significant role in the patient’s survival.22 After administration of intravenous lipid emulsion, haemodynamic stability was achieved. After QTc prolongation was found, propofol and diazepam were started, in which propofol, as a lipid emulsion, could also have acted as an intravenous lipid emulsion.
Immediate, within one to two hours after intake of hydroxychloroquine, treatment with intravenous lipid emulsion, in combination with the usual supportive care known for poisoning with hydroxychloroquine (e.g. intubation, norepinephrine, diazepam and sodium bicarbonate), may have contributed to the survival of both patients.
CONCLUSION
Intoxications with hydroxychloroquine often result in a fatal outcome. Our observations have demonstrated that, besides the usual supportive treatment with norepinephrine, diazepam and mechanical ventilation, the early supplemental use of intravenous lipid emulsion might be a safe and effective treatment to prevent cardiac toxicity after possible lethal intoxication with hydroxychloroquine.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES