KEYWORDS
Giant cell arteritis, vasculitis, arteritis, extracranial
INTRODUCTION
Giant cell arteritis (GCA) is a granulomatous vasculitis of unknown origin, affecting large and medium-sized arteries. Temporal arteritis is a well-known clinical phenotype of GCA, characterised by temporal headache, jaw claudication and visual symptoms and is sometimes referred to as cranial GCA. However, GCA does not exclusively affect the temporal artery or other branches of the external carotid arteries.1-4 In fact, large-artery involvement, mainly aortic, subclavian and vertebral artery, appears to be common in patients with cranial GCA.5 In addition, recent studies have suggested that GCA quite often manifests exclusively in large arteries, i.e. the aorta and proximal branches, with specific signs or symptoms frequently not present.6 This has been referred to as ‘silent’ or ‘extracranial’ GCA.6-8 Diagnostic delay in extracranial GCA, i.e. without cranial manifestations, is a potential source of disease burden and complications.6
The goal of this review is to summarise the current knowledge on large-artery involvement in GCA which, for the purpose of this review, is further referred to as extracranial GCA.
METHODS
A systematic literature search was performed to collect articles on extracranial GCA (figure 1).
For the purpose of this review, and in view of the lack of well-defined terminology for extracranial GCA in the current medical literature, three separate groups were defined prior to the selection of relevant articles, namely:
1. Solitary cranial GCA: patients fulfilling the following:
A) 1990 American College of Rheumatology criteria for GCA
B) Histological proof of temporal arteritis
C) Clinical impression of temporal arteritis (assessed by physician based on typical features, e.g. scalp tenderness, jaw and tongue claudication) all of which lack evidence of large-artery involvement (either clinically or excluded by imaging).
2. Cranial GCA with established extracranial involvement: (i.e. aorta, subclavian, vertebral, carotid, axillary, iliac and femoral artery), which was confirmed by:
A) A typical combination of signs/symptoms, laboratory features and clinical follow-up, or
B) Imaging or biopsy results.
3. Solitary extracranial GCA: evidence of large-artery inflammation, assessed by biopsy or imaging, in patients over 50 years of age without clinically apparent cranial GCA, irrespective of the results of temporal artery biopsy.
Articles reporting on groups 2 and 3 were included. It has to be noted, though, that patients without clinically apparent cranial GCA may still have cranial involvement, which cannot be excluded even with temporal artery biopsy due to limited sensitivity. The main objective of this study was to summarise knowledge on extracranial GCA, irrespective of cranial involvement. Studies on patients with Takayasu arteritis were not included. Although both diseases are sometimes considered to represent a spectrum of the same disease entity, Takayasu patients are, by definition, younger and characteristics of these patients and their disease may be different than for GCA. Epidemiology, histopathology, signs and symptoms, diagnosis, treatment and complications will be discussed. As there is no current literature on pathogenesis, this topic will not be reviewed.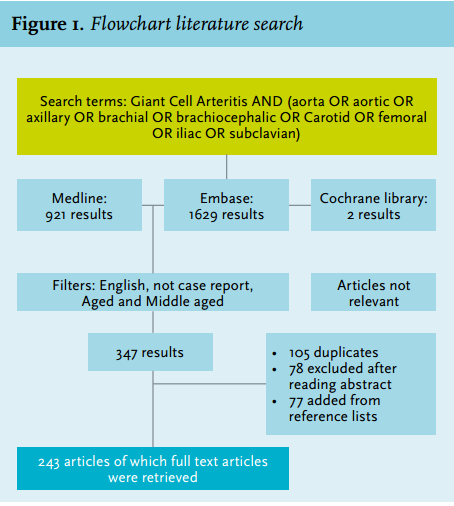
EPIDEMIOLOGY
Cranial GCA with established extracranial involvement
Extracranial involvement in patients with cranial GCA is likely underestimated in early retrospective studies, as patients were not systematically analysed for extracranial involvement.9 If only the symptoms are considered, the prevalence of extracranial involvement was traditionally estimated at 3-15%.10 Clues pointing to a higher prevalence of extracranial involvement were first found in a small post-mortem study showing aortic inflammation in 12 of 13 (92%) patients with temporal arteritis.11 Current estimates are largely based on imaging studies. The highest rate (83%) of extracranial involvement was found in a study using very liberal diagnostic criteria: any degree of uptake of 18-fluorodeoxyglucose (18F-FDG) on positron emission tomography (PET) in large arteries.12 Most prevalence studies, however, have included small numbers of patients and suffer from selection bias, e.g. non-consecutive series, imaging performed at the discretion of the physician or imaging of only symptomatic patients. In addition, several series combine results of extracranial involvement in patients with cranial GCA and solitary extracranial GCA. Table 1 displays an overview of reported prevalences. The aorta and its proximal branches appear to be involved most frequently, although the aorta itself was not studied in all series, namely when ultrasound was used as imaging modality. Lower extremities are less often affected although probably more frequently than previously thought.13,14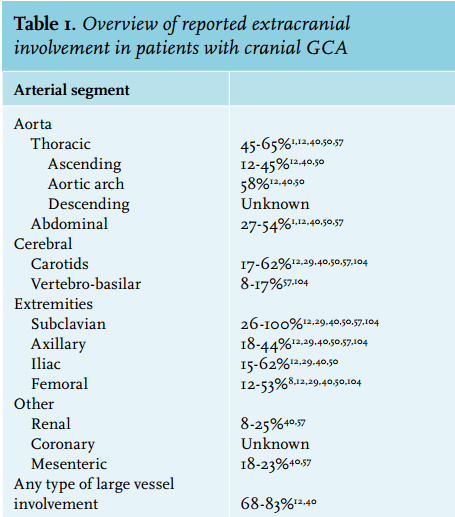
Solitary extracranial GCA
No study has systematically evaluated the prevalence of solitary extracranial GCA. The largest post-mortem population study published (performed in Scandinavia in 889 consecutive patients, six-month selection period, median age 75 (range 39-90) years) suggested a prevalence of extracranial GCA of 1.4-1.7%; only one fifth of these patients had a prior clinical diagnosis of cranial GCA.11 Additionally, series in patients undergoing large-artery surgical procedures, e.g. after aortic dissection or aneurysm, have revealed a high number of cases with extracranial GCA; the prevalence ranged from 1 to 8.4%.4,15-17 Although these series are highly biased by selection, they illustrate that the prevalence of solitary extracranial GCA is higher than previously considered. In addition, extracranial GCA is suspected in 17-25% of elderly patients with fever or elevated erythrocyte sedimentation rate (ESR) of unknown origin.18,19 Few epidemiological data are available to characterise extracranial GCA patients. However, compared with cranial GCA, they seem to be characterised by a higher proportion of women, a younger age at disease onset, and a longer diagnostic delay.6,20,21
Taken together, the true prevalence and incidence of extracranial GCA is unknown, but recent data suggest it may be much higher than the currently estimated incidence of GCA, which is only 1.6-32.8 per 100,000.22,23
Histopathology
Microscopically, extracranial and temporal artery specimens are similar.24 Histological features include intimal thickening and granulomatous inflammation, including lymphocytes and giant cells, often in close proximity to a fragmented elastic lamina (figure 2). In atypical cases, inflammation and medial thickening are moderate and scattered, and dense medial fibrosis is a hallmark.25 Giant cells are found (described, qualitatively, as occurring in a variable number) primarily in the media, and some in the intima.26,27 In the quiescent chronic phase, infiltrates and giant cells become scanty.27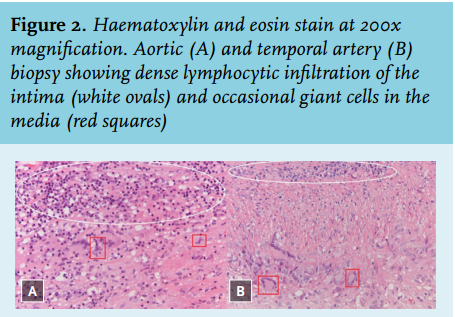
Clinical signs and symptoms
General and cardiovascular signs and symptoms may be encountered in patients with extracranial GCA. The quality of the literature, e.g. small, selected or mixed series, precludes accurate estimates of the prevalence of the various signs and symptoms. However, a couple of conclusions can be drawn.
Patients may be completely asymptomatic and be identified, for example, after an elevated ESR was found during routine examination or after vascular, e.g. aortic surgery.28 An aortic insufficiency murmur may indicate the presence of aortic aneurysm.4
Non-specific symptoms that are considered to be more common in extracranial GCA, with reported prevalences (if known) between brackets, include malaise, fever (10-61%), weight loss (20%), anorexia, polymyalgia (0-40%) and muscle weakness.6,29
Vascular symptoms such as limb claudication, Raynaud’s phenomenon, digital ischaemia, decreased pulses, arterial bruits and signs of cerebral ischaemia are more specific, but are considered less common manifestations of extracranial GCA (prevalences not reported).13,29-31
Symptoms that are more suggestive of cranial GCA such as headache, in some series published as non-specific headache, and polymyalgia rheumatica are reported in 0-10% and 0-40% of cases, respectively.6,29,32
In conclusion, extracranial GCA should be considered in elderly patients presenting with elevated inflammatory markers in combination with either non-specific symptoms or peripheral arterial disease without overt atherosclerosis. Refractory disease should also raise suspicion of extracranial involvement.33
DIAGNOSIS
(Solitary) extracranial GCA is often difficult to diagnose due to non-specific signs and symptoms. Also, affected arteries are frequently inaccessible for biopsy.29 As a result, and also because of a lack of awareness of this disease, an extensive (average up to six months) diagnostic delay may occur, particularly in solitary extracranial GCA, with concomitant morbidity and risk of complications.6,7
Laboratory studies
There is no specific laboratory test for extracranial GCA. Inflammatory parameters (ESR, C-reactive protein) are considered sensitive for GCA, but their exact sensitivity is unknown.3,8,27 In cranial GCA, normal inflammatory parameters are found in up to 4% of cases.34 Whether the data are similar for solitary extracranial GCA is unknown. Whether the level of inflammation is informative, and whether levels in extracranial GCA are higher than in solitary cranial GCA is controversial.6,8,35,36
Imaging
Because signs, symptoms and blood tests are non-specific and affected arteries are difficult to biopsy, the diagnosis of extracranial GCA often relies on imaging. Several imaging modalities are used in clinical practice, all comprising advantages and limitations. An important challenge is to differentiate extracranial GCA from atherosclerotic inflammation.21
Conventional angiography used to be the gold standard for diagnosing extracranial GCA. However, at present, it is no longer indicated as it has been replaced by non-invasive imaging modalities.
Ultrasonography of the affected arteries may reveal homogeneous hypo-echoic swelling of the arterial wall, or stenosis during Doppler ultrasonography (≥ 1.5 mm wall thickness/oedema in the proximal branches of the aorta is regarded to be diagnostic); the thoracic aorta is more difficult to investigate due to the anatomic location below bone and air.29,37 Cut-off values for temporal arteries and aorta have not been described. Areas that are also affected by atherosclerosis are more heterogeneous, and sometimes hyper-echoic.29 In a small study, contrast-enhanced ultrasound was recently suggested to be a marker of disease activity.38
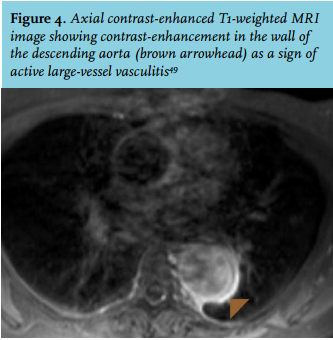
Computed tomographic angiography (CTA) and magnetic resonance angiography display vessel wall thickening, oedema, and mural contrast enhancement (figures 3 and 4).1,39-42 Recently, a protocol for dynamic contrast-enhanced MRI was introduced. The mean extraction of gadolinium, a measure of inflammation, was significantly higher in patients with arteritis compared with controls (suspected of arteritis, but no diagnosis could have been established), and highly correlated with 18FDG uptake.43 This technique has to be further explored.
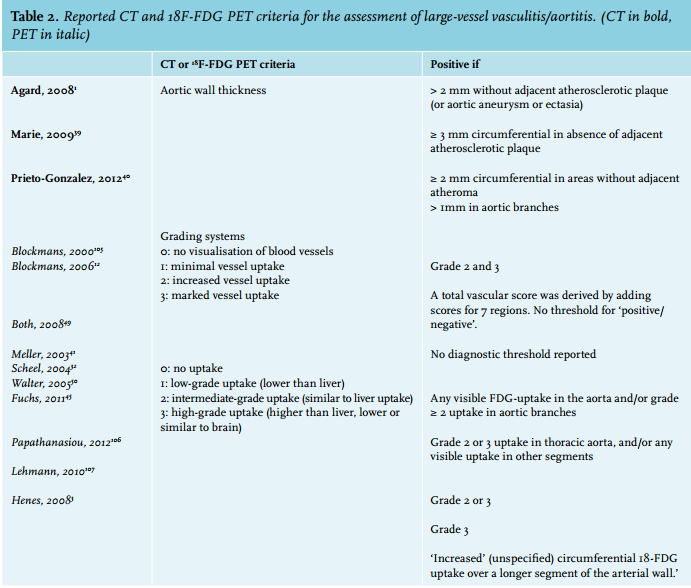
18F-FDG-PET visualises glucose uptake (whole body assessment) by metabolically active cells. Quantitative (metabolic rate of glucose) or semi-quantitative (standardised uptake value) measurements of 18F-FDG uptake in the vessel wall are hampered by partial volume effects, causing overestimated or underestimated FDG uptake, depending on spill-over from or to adjacent regions. Standardised uptake values have been shown to correlate with acute-phase reactants and serum IL-6 concentrations, and may thus correlate to disease activity.44 Nevertheless, due to the aforementioned limitations, a qualitative rather than quantitative assessment of 18F-FDG uptake is generally used (table 2).
A recent study suggested that adding 18F-FDG-PET to routine clinical assessment significantly increased diagnostic accuracy.45 The results of this study should be interpreted with caution as the value of this study may be limited by the fact that the results of 18F-FDG-PET were part of the reference diagnostic criteria.
Because all imaging modalities have limitations, hybrid imaging such as combining 18F-FDG-PET with CT angiography or magnetic resonance angiography may have additional potential for the diagnosis of extracranial GCA. However, such an approach has not yet been studied. 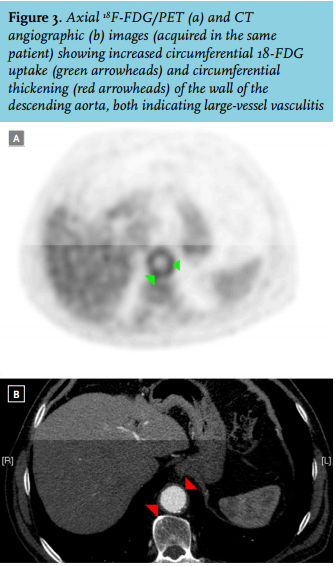
Proposed choice of imaging modality in patients suspected of extracranial GCA
Although all modalities lack solid formal evaluation studies to address diagnostic criteria and diagnostic characteristics, the literature does provide suggestions for a recommended imaging strategy.
Ultrasound (widely available, low costs, no side effects) of the arteries of the proximal arm showed high agreement with MRI and 18F-FDG-PET.29,46 However, ultrasonography is operator-dependent and unable to depict structures beneath bone or air, such as the aorta.
A prospective study suggested that MRI is roughly as sensitive as 18F-FDG-PET(/CT), although more affected vascular segments were detected using 18F-FDG-PET.41 Moreover, 18F-FDG-PET images inflammation rather than morphology, and would thus be expected to better correlate with disease activity.32,41
The most obvious choice of imaging modality in patients will depend on which signs and symptoms initially raised suspicion of extracranial GCA. Three scenarios are most common (figure 5):
• Firstly, patients may present with signs and symptoms suggesting cranial GCA. The initial step is to perform temporal artery biopsy or, depending on local expertise, ultrasonography of the temporal artery and/or proximal branches of the aortic arch. In other cases, or when ultrasound and/or biopsy is normal, 18F-FDG-PET(/CT) seems an appropriate next step, although CTA and MRI are reasonable alternatives. Larger, prospective, studies should compare which modality has the best diagnostic accuracy and prognostic significance in these cases.
• Secondly, extracranial GCA may be suspected in patients presenting with large-artery disease, either with or without elevated inflammatory parameters.47 In such cases, CTA or MRI will often be available as part of the diagnostic work-up, and may therefore be used.
• Thirdly, older (i.e. > 50 years of age) patients may present with constitutional symptoms (fever, night sweats, etc).47 The differential diagnosis in these patients is broad, including extracranial GCA, infection and cancer, all of which may be detected by 18F-FDG-PET(/CT), after routine tests have been non-diagnostic.19
Regardless of the clinical scenario, the sensitivity of CTA, MRI and 18F-FDG-PET for the detection of extracranial GCA decreases during corticosteroid treatment. 48-50 Therefore, we recommend that imaging is performed prior to or as soon as possible after the initiation of immunosuppressive treatment: i.e. within 24 hours, although this is merely experience based. Conceivably, this is particularly relevant for 18F-FDG-PET. If imaging studies are ordered when treatment has started and systemic inflammation has subsided, thus decreasing the sensitivity of 18F-FDG-PET, morphological studies (MRI or CTA) may be the best option.12,32
Finally, variability in diagnostic criteria used in CTA, MRI and 18F-FDG-PET illustrate the need for standardisation of diagnostic and classification criteria (table 2). Currently, the American College of Rheumatology and European League Against Rheumatism are developing a new set of diagnostic and classification criteria for primary systemic vasculitides (clinical trials: NCT01066208). 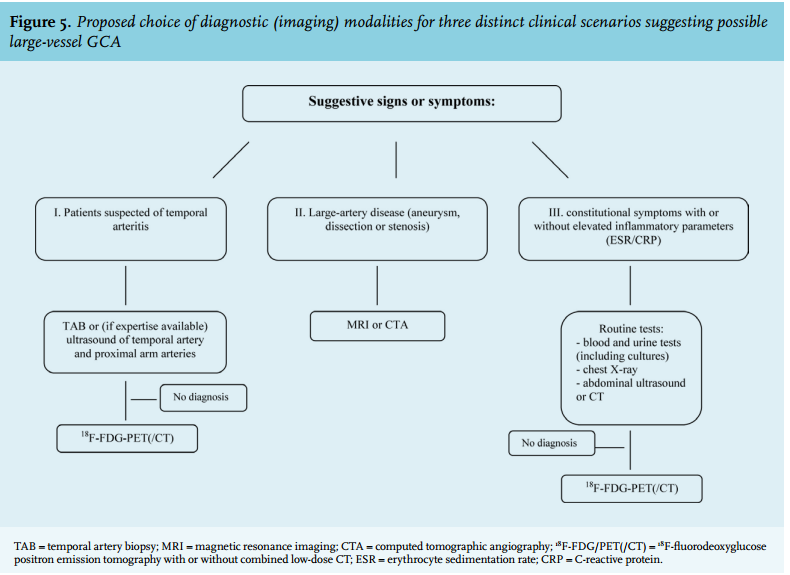
Biopsy
Large arteries are usually inaccessible for biopsy unless vascular surgery is required.51 On routine clinical biopsy, temporal arteries are infrequently involved in solitary extracranial GCA.6,51 The sensitivity of an appropriately obtained (at least 1-1.5 cm during surgery, > 7 mm after fixation) temporal artery biopsy in extracranial GCA may be no higher than 58%.6 In view of reported sensitivities of 56-91% in clinically apparent cranial GCA patients, this is not surprising.52,53 Sensitivity probably depends on the presence of symptoms suggestive of temporal arteritis.53 Despite the risk of false-negative results, some recommend temporal artery biopsy in patients with suspected solitary extracranial GCA, as a positive result is highly specific for GCA. One could argue, however, not to biopsy when imaging results are highly suggestive of extracranial GCA as a negative biopsy by no means excludes GCA, certainly not in large arteries.
The influence of steroids on the results of temporal artery biopsy is undetermined in extracranial GCA. Aortic biopsies of patients treated with low-dose steroids prior to surgery showed persistent features of aortitis.54 Prolonged steroid use tends to render pathological features less specific. Sensitivity may, however, be largely maintained as disturbed media anatomy and fragmentation of the internal elastic lamina persist.27
DIFFERENTIAL DIAGNOSIS OF LARGE-VESSEL VASCULITIS
When large-artery inflammation is suspected, e.g. after imaging, the differential diagnosis includes more than just GCA, particularly in the absence of cranial GCA symptoms. Both primary and secondary large-vessel vasculitis have to be considered. Primary large-vessel vasculitis mainly consists of GCA and Takayasu arteritis. Apart from age, a difference in systolic blood pressure of > 10 mmHg and arm or leg claudication are suggestive of Takayasu, whereas myalgia is more common in GCA.32 Histopathology is largely identical, and giant cells occur in both conditions.55,56 In addition, imaging characteristics are similar.57
Secondary large-vessel vasculitis is less common and may be caused by infection, such as HIV, syphilis, tuberculosis, or hepatitis, or may occur in systemic inflammatory disease, such as rheumatoid arthritis, Behçet’s disease, Cogan syndrome, relapsing polychondritis, systemic lupus erythematosus, sarcoidosis or IgG4-related aortitis.56,58,59
COMPLICATIONS AND PROGNOSIS
Most of the current knowledge on this topic is derived from studies in patients with cranial GCA, predominantly in those without prior evidence of extracranial involvement. Nevertheless, as extracranial complications did develop in these patients, inflammation in these vessels was considered to be present. The most frequent complication is arterial stenosis.60 However, more serious complications (aneurysm or dissection, the incidence being higher than arterial stenosis when both are combined) may occur. Moreover, sudden death from aortic rupture may be the first disease manifestation.20 The cumulative incidence of extracranial complications has increased significantly in recent years, most likely due to a greater awareness and an increased use of imaging techniques.61
Ischaemia
Aortic arch syndrome was already reported as a complication of GCA in 1938.62 Aortic arch syndrome and aortic aneurysms may, in rare cases, occur simultaneously.20,63 Stenosis of arteries supplying the upper extremities occurs in 5-45% of GCA patients with extracranial involvement.29,60,63,64
Ischaemic stroke occurs mainly due to vertebrobasilar artery involvement, although carotid arteries may also be affected. Approximately 3-7% of patients experience stroke, usually occurring between the onset of symptoms and four weeks after initiating corticosteroids.65,66 Smoking adds to the risk of vertebrobasilar stroke.65 Stroke may, however, also be due to cranial involvement of GCA.
Whether the risk of acute myocardial infarction is increased is unclear. In one study, 38 of 167 (23%) patients developed acute myocardial infarction after GCA or polymyalgia rheumatica was diagnosed, with male sex and presence of hypertension as additional risk factors.67
A large study showed that, after adjustment for cardiovascular risk factors, GCA patients had a higher risk of peripheral vascular disease (HR 1.85, 1.45-2.36) and cerebrovascular accidents (HR 1.71, 1.27-2.29) when compared with non-GCA patients.68 In addition, GCA was an independent risk factor for serious cardiovascular events.69
Aortic aneurysm
In a relatively small follow-up study, the only study performed to date in patients with established extracranial involvement, both male and female GCA patients developed larger ascending aortic diameters than matched controls.70 Clinical symptoms relating to aortic aneurysm occur in only 3-13% of cases.71 The overall prevalence of aortic aneurysms is undetermined and probably ranges between 0-27%.64,72,73 Intriguingly, the geographical distribution of GCA incidence resembles that of aneurysmatic disease.73,74 The diagnosis of aneurysmal disease is usually established within the first 4-5 years after the diagnosis of GCA.60,64,71,73,74 Younger age, male sex, polymyalgia and hypertension are additional risk factors.60,64,73,74 The thoracic aorta is most often affected.75 Thoracic aortic aneurysms occur roughly equally often in the proximal ascending aorta, the aortic arch and the descending aorta.15 It has been suggested to screen all patients with temporal arteritis for large-artery complications (i.e. yearly CT scan or chest X-ray and abdominal ultrasound), but the yield of such a strategy is undetermined.9,54,76
Finally, distal aortic events such as abdominal aortic aneurysms develop more frequently in patients previously diagnosed with large-vessel GCA.28
Relapse and inflammatory markers (ESR/CRP) were negatively correlated with the development of aortic structural disease in one study.76 These findings are remarkable as a recent study showed a higher number of relapses in patients with extracranial GCA established by imaging, suggesting these patients would be more prone to extracranial complications.77
Aortic dissection
Dissection occurs more often in GCA. The exact incidence is, however, unclear.78 A near-complete disruption of the elastic lamina weakens the aortic wall and probably renders it prone to dissection.54 Hypertension and diagnostic delay increase the risk of dissection.60 Dissections occur at a median of 2.5 years after GCA diagnosis.9
Mortality
GCA patients presenting with acute aortic pathology as the first clinical manifestation have a high mortality rate (44-80%), whether or not they have previously established extracranial involvement.17,61,74,79 Mortality is markedly increased in GCA patients in whom thoracic aortic dissections and aneurysms develop (HR 3.4; 95% CI 2.2-5.4), whereas increased mortality has not been established in patients developing other large-artery complications.61,80 In addition, a retrospective study showed that patients with extracranial GCA (aortitis) had more vascular causes of death and more vascular events, including stroke, than GCA patients without aortic involvement.81 Mortality due to ischaemic heart disease was higher in patients with GCA than in patients with ischaemic heart disease without GCA (HR 3.42; 95%-CI 1.85-6.33).82
TREATMENT
Immunosuppressive therapy
In the absence of randomised clinical trials, the need for immunosuppressive therapy for extracranial GCA is unproven. Current data do not support a more aggressive approach as long-term outcome of patients with ‘isolated’ GCA is considered to be good.56 Nevertheless, no prospective trials have been performed in such patients. A more aggressive, pre-emptive treatment is supported by several non-randomised, non-controlled studies. In a study of 36 extracranial GCA patients, 11 received steroids and developed no new aneurysms, whereas six of 25 untreated patients did.83 In our clinical experience, general symptoms such as malaise, fever, myalgia, and anaemia often subside almost instantly in extracranial GCA patients after steroid treatment. One recent, prospective trial also showed improvement of CTA signs of vasculitis one year after treatment with glucocorticoids.84
If treatment is indicated, patients are often subjected to the same regimen as cranial GCA patients. Although there is no generally accepted regimen, it is common to start with a prednisone dose of 40-60 mg (or 1 mg/ kg).85-87 Gradual tapering is needed: 5 mg every 1-2 weeks until a dose of 10 mg/day is reached, after which smaller steps are indicated. There are no validated biomarkers, neither chemistry nor imaging, to assess response or relapse.87,88 The duration of therapy is highly variable, with some patients experiencing a chronic relapsing course.86 Osteoporosis prophylaxis and gastric protection should be considered.85,88
Several disease-modifying anti-rheumatic drugs and biological agents have been investigated in patients with cranial GCA, and may be considered in extracranial GCA if corticosteroids are not tolerated or in steroidrefractory cases.89 Methotrexate, infliximab, etanercept azathioprine, cyclophosphamide, mycophenolate, leflunomide and – more recently, showing great potential – tocilizumab have been described in patients with temporal arteritis without known large-vessel involvement, largely with conflicting results.59,87,90-97
Surgery
Reconstructive surgery is not recommended during active inflammation, since most patients will respond to high-dose corticosteroids.98 Furthermore, vascular anastomoses tend to occlude when performed during active disease.31,99
The technical success rate of upper limb revascularisation ranges from 50%, in case of occlusions, to 100% in case of stenosis.100,101 Recurrent lesions mainly develop in territories of initially long-segment ( > 3 cm) lesions.102
Repair of GCA-related aortic aneurysms seems safe and efficacious. An open procedure is preferred in patients with minor comorbidity and low expected mortality.103 Patients undergoing repair of ascending aortic aneurysms secondary to giant cell arteritis should undergo life-long screening evaluations of the remaining aorta, as a significant percentage require intervention for more distal disease.15,28
AREAS OF UNCERTAINTY
Our knowledge on extracranial GCA has expanded substantially over the last years. There is no internationally accepted definition for extracranial GCA, and heterogeneity in definitions complicates comparison of studies. Although it is most likely that cranial and extracranial GCA are two entities in a spectrum, clear definitions would facilitate scientific progress in this field.
Despite increased awareness, the current literature on extracranial GCA is still limited. Several uncertainties remain, two of which we believe deserve a particularly high priority.
The first pertains to diagnosis and involves the question of which imaging modality is preferred, and how imaging can contribute to the establishment of a diagnostic reference standard, given the limitation that biopsy of affected arteries is often impossible. For this purpose, studies prospectively comparing imaging modalities need to be performed. In addition, standardised criteria for the reporting of large-artery inflammation need to be established for all image modalities.
Secondly, there is controversy whether or not to treat all cases of solitary extracranial GCA and, if so, whether the same treatment protocol as for cranial GCA applies. This controversy partly relates to the unknown incidence of complications in (solitary) extracranial GCA, whether this differs from patients with cranial GCA in whom extracranial involvement was excluded by imaging, and the potential of immunosuppressive therapy to prevent these complications. Hence, studies need to address whether large-artery complications develop more frequently during long-term follow-up in patients with extracranial involvement at GCA diagnosis or solitary extracranial GCA, as compared with patients in whom the disease appears to be restricted to the temporal arteries.
DISCLOSURES
The authors have nothing to disclose.
REFERENCES