Some years ago, there was a lot of discussion about a shortage of emergency physicians in the Accident & Emergency (A&E) departments and the poor training given to house doctors fulfilling this function in the evening and night hours.1
The report ‘Spoedeisende hulp: vanuit een stevige basis’ (‘A&E Department: On a firm basis’) of the workgroup ‘Kwaliteitsindeling SEH’ (‘Quality Classification in the A&E Department’) from 2009 describes the minimal mandatory quality requirements to run an A&E department. The Ministry of Health then concluded that no single Dutch A&E department completely fulfilled these criteria. It was agreed that the Inspection for Health Care should introduce more stringent control on the presence of properly trained personnel. Training in acute medicine in accordance with the ABCDE (Airway-BreathingCirculation-Disability-Exposure) systematics became mandatory. Such a training program has been described for the interns of the department of internal medicine in the Academic Medical Centre Amsterdam2 and a comparable course was set up in the Leiden University Medical Centre by the A&E department.3
Training in acute medicine, a task for the ICU
In a recent article in Intensive Care Medicine4 it was shown that, in the Netherlands, contrary to earlier non-evidence based reports, care on smaller ICUs was as good as care on medium sized and larger ICUs; this includes the sickest and ventilated patients. The ‘smaller’ ICUs (with a median size of seven ventilation beds, which is not small at all with respect to the rest of the world) have a number of other important tasks next to their core business, intensive care treatment. They run the Medical Emergency Team (MET) thus decreasing the number of in-hospital resuscitations, ICU admissions, ICU length of stay and hospital mortality. Furthermore, they manage A&E admissions in patients who are unstable or critically ill and finally, they organise the training of nurses in emergency medicine and intensive care medicine. Consequently, it seemed logical to let the ICU department organise the training in acute medicine for all interns being engaged at any moment on the A&E department. In the Slotervaart Hospital we developed an introductory course which was mandatory for all starting interns. A similar course in the Amsterdam region, organised by the ICU team, is being offered by the Spaarne Hospital in Hoofddorp.
Our course was implemented by the intensivists in 2010, and by now has been given 21 times (four times per year), in cooperation with different hospital consultants. Each participant receives the course book ‘Medische spoedsituaties’ (‘Medical Emergencies’) (T.J. Olgers, M. Oosterloo, J.C. ter Maaten) and a pre-test with 50 corresponding multiple choice questions six weeks before the start of the course. A literature study and pre-test have to be done at home before the start of the course and pre-tests are collected and corrected at the beginning of the course.
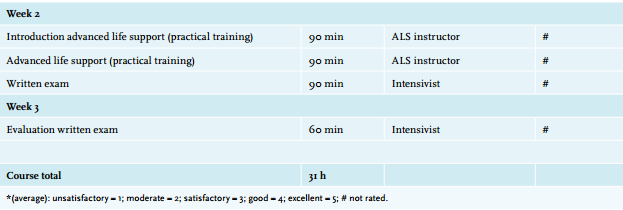
The course itself consists of three days of training, with three hours of theoretical lessons per half-day session. At the end of each session two patient cases are managed and discussed with an intensivist in small groups of three to four participants to put the acquired knowledge into practice. At the end of the third day each participant concludes with a practical exam by managing one virtual critically ill A&E patient case on his own. In week two all participants follow a resuscitation training on an Advanced Life Support simulator under supervision of a certified trainer. After seven days of self-study a final theoretical exam, consisting of 50 multiple choice questions, is completed. This exam is evaluated and discussed with all participants in week three. The total number of lessons comprises 31 hours and passing both (practical and theoretical) exams is mandatory to obtain the course certificate. Table 1 shows the course program with average rating by the participants.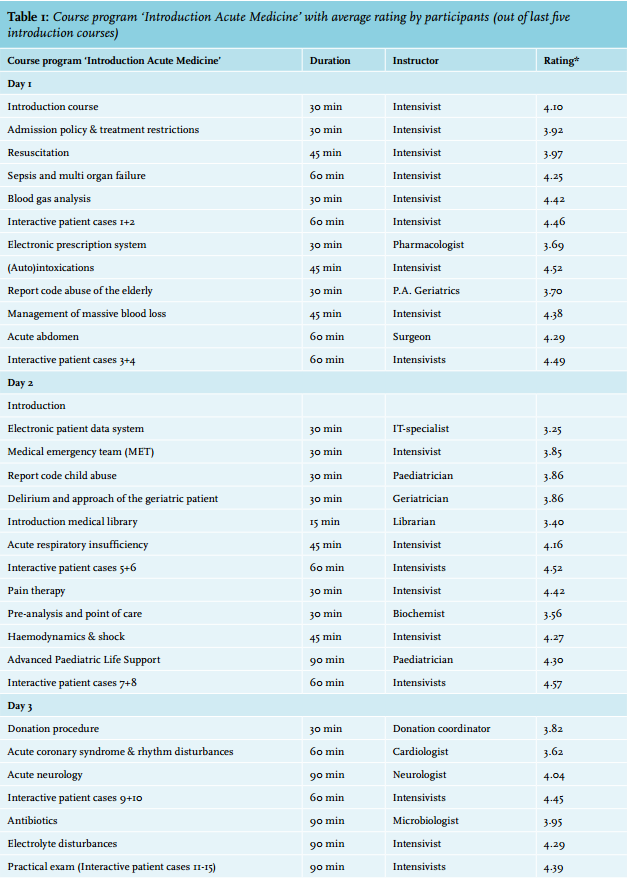
Aim of the course
This course aims at making the starting interns confident with all facets of acute medicine and to teach them the ABCDE principle, internalise it and put it into practice.
In our view, the advantage of this custom-made course, contrary to a national (ATLS) two-day course, is to familiarise the interns with the local consultants and to make them proficient in the hospital guidelines. This, in our opinion, lowers the threshold to consult consultants and reduces the need for calling in the Medical Emergency Team (MET). This increases effectivity and safety of the emergency patient admission process. More specifically, the course is longer than the ATLS course and includes non-trauma cases, thus offering a broader and more in depth knowledge to the participants.
Each course is being evaluated and the participants are enthusiastic about the small study groups, the low threshold atmosphere and the practical design of the course. Since 2013 evaluation is done via an online system (SurveyMonkey). The course corresponds well with the theoretical knowledge acquainted during the study, being consistently rated as ‘precisely corresponding with present knowledge’ of the participants.
In the future, interactive patient cases, rated as the most valuable part of the course, will be simulated in a real-life A&E environment, with a simulation mannequin and full monitoring. We will evaluate the effect of this measure after one year.
Naturally a four-day course does not make a starting intern fully competent in acute medicine. For this reason it is important that the acquired theoretical knowledge is put into practice and the intern is supervised when dealing with acutely ill patients. This supervision in our hospital is offered by the admitting consultant, and in critically ill patients by the intensivist who is readily available for consultation.
The intensivist organises the course and indeed carries out most of the lectures, which corresponds well with his central role in caring for the acutely ill patient. This creates uniformity within training and patient treatment. It gives the ICU department a central role in the hospital structure.
CONCLUSION
The four-day introductory course Acute Medicine is being received very positively by the participants. By involving the hospital consultants in this course, an effective and safe approach to treating the acutely ill patient is being created. In this way, this course fulfils the requirements of the Ministry of Health.
REFERENCES