KEYWORDS
Birth weight, epidemiology, pregnancy
INTRODUCTION
Gestational diabetes mellitus (GDM) has been associated with an increased risk for perinatal complications such as pregnancy-induced hypertension, prematurity, caesarean section, shoulder dystocia and macrosomia.1-4 Pregnancy is an insulin-resistant state, in part mediated by the action of human placental lactogen, human chorionic somatomammotropin, growth hormone and corticotrophin-releasing hormone.5,6 The diabetogenic placental hormones increase with placental size and, therefore, gestational diabetes is usually not present until the second or third trimester of the pregnancy.5
Several reports from the Netherlands confirmed a high frequency of complications in pregnancies of diabetics.7-10 Data from an epidemiological study in the Netherlands suggested that there was an important ethnic difference in foetal mortality with significantly elevated risk in nulliparous women of South Asian and African origin.11 A possible explanation was that non-Western women have cultural and educational barriers, which influence the access to regular care or its effectiveness.11 There is only limited information on pregnancy-related complications in ethnic minorities with diabetes in the Netherlands. Moreover, these studies were only carried out in diabetes mellitus type 2 (T2DM) patients.7,8 In this study, we aimed to compare perinatal outcomes in women with GDM between different ethnic groups.
METHODS
Patients
The local medical ethics committee of the Maasstad Hospital in Rotterdam approved this study. Consecutive patients with a diagnosis of GDM, who visited the outpatient clinic for Diabetes Care of the Department of Internal Medicine of the Sint Franciscus Gasthuis in Rotterdam between 2010 and 2013, were included. Women were referred to our clinic and were first treated with lifestyle measures. In case of insufficient response to lifestyle intervention, patients started insulin therapy. All diabetic patients are extensively evaluated during the regular multidisciplinary meetings once a month, which were attended by obstetricians, internist-endocrinologists, dietitians and specialised diabetes nurses. The department serves as a referral centre for pregnant women with diabetes in the Northern part of the Rotterdam region.
Maternal, foetal and neonatal data were recorded by each professional following protocols and data were entered into the database. Patients had to have a diagnosis of GDM, defined as an abnormal 75-gram oral glucose tolerance test (OGTT). Reference values for the OGTT were < 7.0 mmol/l for fasting glucose and < 7.8 mmol/l two hours after glucose load. Patients who were referred to our centre, but had their delivery in another centre or at home, were asked permission to obtain the birth data from the general practitioner. If no permission was given, data for these subjects were not included in the final analysis. Multiple births were also not included in the analyses.
Outcome measures
Maternal characteristics
Maternal age in years and body mass index (BMI) in kg/ m2 before the pregnancy were collected as continuous data. Gestational age at first antenatal visit in weeks was counted from the first day of the last menstruation. The presence of chronic hypertension was recorded based on the use of specific medication and medical history. Chronic hypertension in pregnancy was defined as hypertension that had been diagnosed before 20 weeks of gestation and if it persisted three months after delivery.12
Conception by means of in vitro fertilisation (IVF) was recorded separately. The referring physician was also recorded (general practitioner, obstetrician or internist). Ethnicity was divided into six groups: Moroccan, Turkish, Caucasian, Surinamese-Creole, Surinamese-Hindu and Miscellaneous. Finally, diabetes treatment was scored as diet only or diet and insulin. Insulin regimens were defined as receiving long-acting insulin once a day and/or short-acting insulin once, twice or three times a day.
Obstetric complications
Gravidity and parity were registered as categorical data. The duration of pregnancy was recorded in weeks. Prematurity was defined as delivery before 37 weeks of gestation. The mode of delivery was recorded as normal, assisted or as caesarean section, and could be either spontaneous or induced. The indications for induction of labour were gestational age over 38 weeks in the case of inadequate control of the diabetes or unstable serum glucose levels, and a deteriorated condition of the foetus or mother. Caesarean section was carried out when an estimated weight above 4000 grams was established, or based on obstetric history or location or condition of the foetus.
Pregnancy-induced hypertension (PIH) was diagnosed as systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg after 20 weeks gestation, measured twice, in a previously normotensive woman. Preeclampsia was classified as the combination of PIH with proteinuria (≥ 300 mg/24 hours). HELLP syndrome was classified as the combination of haemolysis, elevated liver enzymes, and lowered thrombocytes.13
Complications during delivery were recorded as shoulder dystocia,14 episiotomy or more than 1000 cc blood loss.
Neonatal outcome
Miscarriage was defined as spontaneous abortion up to a gestational age of 24 weeks. Foetal perinatal mortality was defined as death after 28 weeks of gestation or in the first seven days postpartum. Birth weight was recorded as a continuous variable (in percentiles), according to the Netherlands perinatal registry which also takes into account the number of pregnancies, gender and ethnicity.15 Macrosomia was defined as birth percentile ≥ 90 and dysmaturity as birth percentile ≤ 10.15 Congenital malformations were recorded as fatal, potentially life-threatening, likely to lead to serious handicap or as a major cosmetic defect, or requiring major surgery.9 Neonatal hypoglycaemia was defined as a capillary blood glucose < 2.6 mmol/l in the infant in the first 24 hours after birth. We used that definition because abnormalities of the neonatal brain on magnetic resonance imaging have been detected if the plasma glucose falls below that value.16 Hyperbilirubinaemia was recorded if the newborn required at least one period of phototherapy.
Laboratory analyses
Glycaemic control was established by HbA1c measurements. The target value of HbA1c was between 20 and 42 mmol/mol. HbA1c values were recorded as pre-conceptional and at trimester 1, trimester 2, trimester 3 and postpartum. Because GDM is generally diagnosed in trimester 2 or 3, only the HbA1c values of trimester 2, 3 and postpartum were used for analysis. In the case that more than one HbA1c value was available in the trimester, the mean HbA1c value of that trimester was used.
HbA1C concentrations were only determined if the patient required insulin. In most women treated with lifestyle, only self-measurement of capillary glucoses was recorded. In the years 2010 and 2011, most women with GDM were referred based on an increased capillary glucose day curve. From the year 2012 an OGTT was used for diagnosing GDM following guidelines.17 Women were screened at their first antenatal visit. The 75-gram OGTT was performed if a random and fasting venous glucose was determined above 6.1 mmol/l and in women with risk factors. Women with a history of GDM underwent an OGTT at 16 weeks of pregnancy and between 24 and 28 weeks of pregnancy. Women with risk factors for GDM also had an OGTT between 24 and 28 weeks of pregnancy. Risk factors for GDM are: history of GDM, BMI > 30 kg/m2 at the first antenatal visit, previous child with a birth weight > P95 or > 4500 gram, first-degree family member with diabetes, certain ethnic groups where diabetes is common (Hindus, Afro-Caribbeans, women from the Middle East, Morocco and Egypt), unexplained foetal death in the history or polycystic ovary syndrome. Venous samples were obtained for glucose measurements at baseline and two hours after glucose load. Reference values for glucose are < 7.0 mmol/l at baseline and 7.8 mmol/l at two hours. If one of these values was increased, the diagnosis GDM was established and lifestyle measures were taken, followed by insulin therapy when necessary. Short-acting insulin was initiated if postprandial values were > 6.7 mmol/l and long-acting insulin was prescribed if fasting glucose was above > 5.3 mmol/l.
All laboratory measurements were carried out in our clinical chemistry laboratory following standard procedures.18 For the OGTT, blood samples were obtained fasting and two hours after ingestion of 75 grams of oral anhydrous glucose. Blood was drawn from a peripheral vein of the forearm. Some women were referred by a different hospital or a midwife and those data were used when available.
Three months after the delivery, HbA1c was again determined in all women who used insulin during pregnancy.
Statistical analysis
Statistical analysis was carried out using SPSS version 22.0 (IBM Corp, Armonk, NY, USA). Results for continuous variables are given as mean and standard deviation, differences between groups were tested by analysis of variance, post-hoc analysis was tested by Fisher’s least significant difference test. For categorical variables, data are given as frequencies and percentages, and Chi-square test was used to evaluate differences between the groups. P-values < 0.05 were considered to be significant. To evaluate a relationship between HbA1c values during pregnancy and hypoglycaemias of the newborn within 24 hours after birth, Spearman correlation analyses were carried out.
RESULTS
General characteristics
A total of 388 pregnancies of women with GDM were recorded. The number of women increased gradually due to the intensified screening programme. Over the four years there were 388 pregnancies, with one miscarriage (0.3%); therefore, 387 were included.
Characteristics and outcome based on ethnicity
Table 1 shows the general characteristics of the women with GDM based on ethnicity. Caucasians formed the largest group followed by Moroccans. BMI before pregnancy was highest in Surinamese-Creoles, followed by Turkish and Moroccan women.
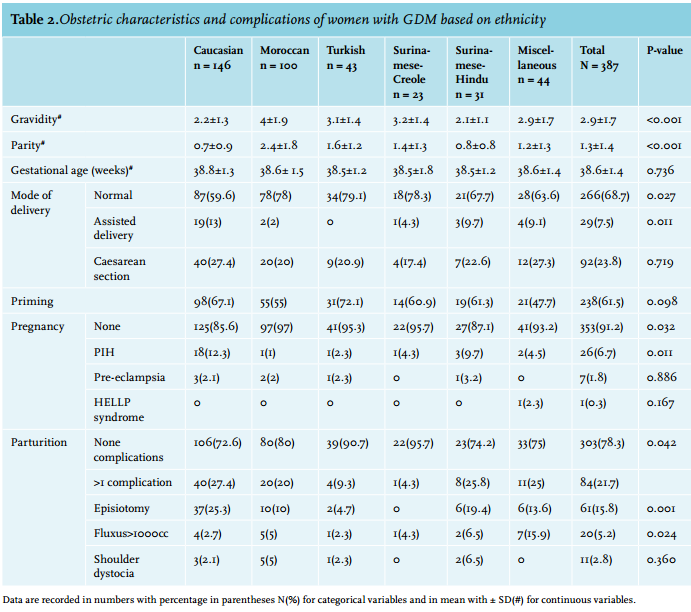
Gravidity and parity rates were highest in Moroccan females, gravidity was lowest in Surinamese-Hindus and parity was lowest in Caucasian women. PIH occurred most frequently in Caucasian and Surinamese-Hindu women. A normal delivery was most frequently observed in the Moroccans, followed by the Turkish and caesarean section was most frequently carried out in the Caucasian group. Assisted delivery differed significantly between the ethnicities, due to a high frequency in Caucasians and it did not occur in Turkish women. An episiotomy was more frequently performed in Caucasian females. Table 2 shows the obstetric characteristics and complications of the women, based on ethnicity.
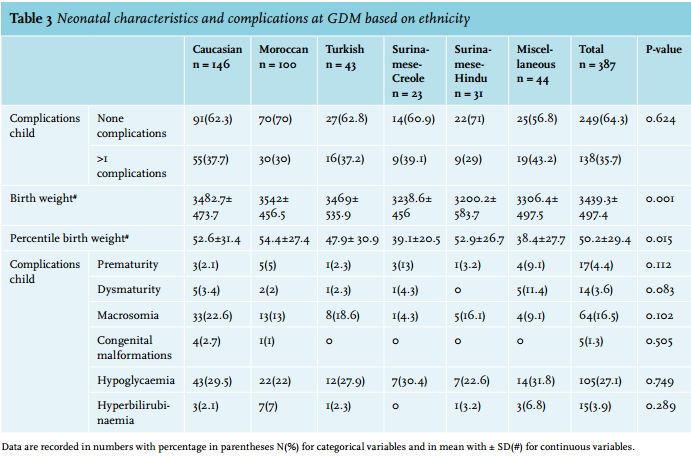
Neonatal characteristics and complications based on ethnicity are given in table 3. Birth weight was highest in newborns from Moroccan mothers and lowest in Surinamese-Creole and Surinamese-Hindu newborns. Birth weight percentiles were highest in Moroccans, followed by Surinamese-Hindu newborns. Birth weight in the miscellaneous group of newborns was in the lowest percentile. There were no significant differences between the ethnicities and neonatal complications.
HbA1c changes during pregnancy
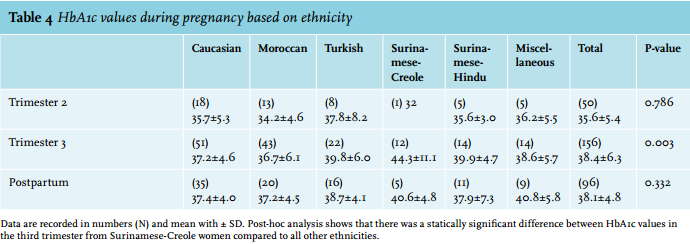
Table 4 shows the course of HbA1c during the pregnancy for each ethnicity. The data for HbA1c were incomplete and only the HbA1c values of trimesters 2, 3 and postpartum were used. Caucasian, Moroccan, Turkish, Surinamese-Hindu and Miscellaneous women showed almost the same trend with almost equal values in trimesters 2, 3 and postpartum. Only Surinamese-Creole women showed a different pattern with a higher mean HbA1c value in trimester 3. Univariate correlation analyses using Spearman correlation coefficients between HbA1c and hypoglycaemia showed only a trend in the third trimester with a Spearman’s rho of 0.176 (p = 0.052). 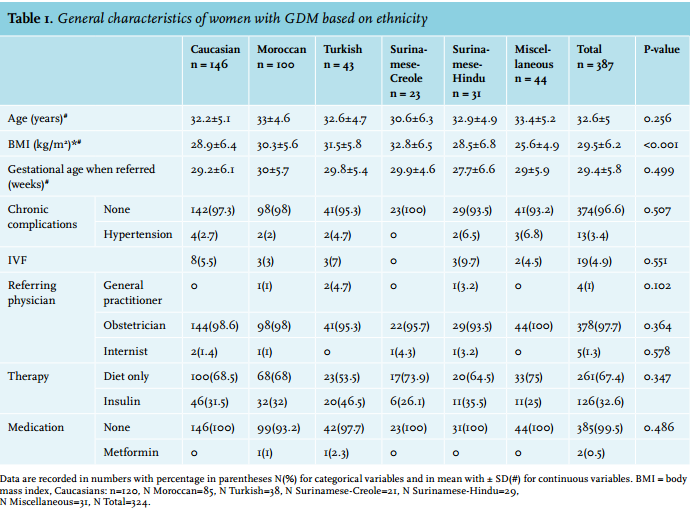
DISCUSSION
This single-centre, retrospective study performed over four years shows the outcomes of pregnancies of women of different ethnicities with GDM. There were no major differences between the ethnic groups in neonatal complications related to diabetes. However, there was a significant difference in (percentile) birth weight and mode of delivery.
To the best of our knowledge, this is the first study in the Netherlands comparing pregnancy outcomes in women with GDM of different ethnicities. Previous studies in the Netherlands reported differences in T2DM and ethnicity.7,8 Both studies showed no differences in perinatal outcomes between native and non-native (Moroccan) women.7,8
However, the caesarean section rate was higher in native Dutch women.8 The authors concluded that in a setting of easy access to, and compliance with the local healthcare system, outcome in non-native women can be similar to that in native women. This easy access to care might be positively affected by the fact that medical care in the Netherlands is fully reimbursed with insurance coverage for basically all inhabitants, resulting in an absence of any financial barriers to receiving medical care.8
Studies from other countries in women with GDM included other ethnicity groups.3,4,19-23 Hispanic neonates in the USA were more likely to experience adverse neonatal outcomes.4,19 Afro-Caribbean women, comparable to the Surinamese-Creole women in our study, were more likely to have a normal delivery in comparison with Caucasian women.24 Our study confirms these results. A study from New York suggested ethnic variations, with a relatively higher incidence of complications in Caribbean, Sub-Saharan African, and African-American women, while North African, South Central Asian, and Chinese women showed a relatively smaller incidence of complications but a higher baseline risk of GDM.3
In the four years of our study, the number of patients included each year increased from 64 in 2010 to 153 in 2013. This was mainly due to changed guidelines for identification of GDM, which were introduced in our hospital in 2012.17 Furthermore, GDM prevalence is increasing in many populations worldwide concomitantly with the observed increase in T2DM.25 The increasing age of pregnant women and the increased number of minority immigrants have likely contributed to this increase in prevalence.1,25-27
PIH was significantly different between the ethnicities in our study, with the highest rate in Caucasian women. In another study, Caucasians also had the highest rate of PIH.19 Episiotomy was not recorded in previous studies. The higher rate of episiotomy in Caucasians and Surinamese-Hindu ethnicities and the increased frequency of assisted deliveries and caesarean sections in Caucasians may be associated to the observed lower parity in these groups. Indeed, it has been published that a higher number of deliveries in women is associated with a higher rate of normal deliveries.8,28
Neonatal outcome
We expected that the outcome in non-native women with diabetes would be poorer as compared with Caucasian women. There was a significant difference in birth weight and percentile birth weight. Remarkably, children from Surinamese-Hindu mothers had the lowest birth weight, but when considering the percentile, they had the highest mean percentile after Moroccans. This can be explained by the fact that we used special birth weight curves for Hindu children. A study from Australia also included the Pacific Islanders ethnic group and they had a mean birth weight of 3700 gram with a mean percentile of 70.5.22
The stillbirth rate in our study (0.3%) cannot be compared with other studies due to a lack of data in the literature.
We have to take into consideration that miscarriage is difficult to confirm and often occurs in the first weeks of pregnancies. Perinatal death after 28 weeks of gestation did not occur in our study.
Congenital malformations are a common complication in the offspring of women with T1DM or T2DM.7,9,24,29-38 The increased risk of anomalies is predominantly for cardiovascular defects, followed by musculoskeletal and central nervous system anomalies.33,38,39 For GDM, risk of congenital malformations is not an issue because they arise in the first trimester of the pregnancy.
Neonatal hypoglycaemia rates in our study were high in comparison with a recent study were the authors compared untreated and treated GDM. There were no major differences, but Hispanic women had more frequent neonatal hypoglycaemia.4
Limitations
Several limitations of this study should be noted. Firstly, the number of patients in some ethnic groups such as Turkish, Surinamese-Creole and Surinamese-Hindu were small. Secondly, women entered care at different gestational ages. GDM was often referred in the third trimester, because the diabetes usually reveals at that stage. However, there were some women who were already referred with elevated disturbed glucose values in the first trimester. Since the diabetes was discovered during pregnancy, the diagnosis of GDM was established by definition, but one has to take into consideration that some women may have had a longer existing T2DM.
National database
In our hospital there is a structured, multidisciplinary approach for the pregnant women with diabetes mellitus. Therefore, it was expected that the results would be better than previous reports where care for these women was less strict. The Netherlands Perinatal Registry recently published the trends in deliveries from 1999-2012.40 The mode of delivery in the national database reports 74.5% normal deliveries, 10.2% assisted deliveries and 15% caesarean sections, but data on ethnicity are not available. The total percentage of prematurity was 7.7% in the total population of pregnant women. It is only in the Surinamese-Creole ethnicity and miscellaneous group that prematurity occurred more frequently. The rate of congenital malformations in newborn babies of women with GDM was comparable to the normal population of pregnant women in all the six types of ethnicities.41 Other perinatal outcomes such as macrosomia or hypoglycaemia were not recorded in the Netherlands Perinatal Registry.
Predictive variables
In a study of pregnancies complicated by gestational diabetes or impaired glucose tolerance, in the late second and early third trimester, maternal BMI and macrosomia in a previous pregnancy seemed to have the strongest influence on foetal growth, while maternal fasting glycaemia during 32-35 weeks was the strongest predictor of accelerated growth in the late third trimester.42
Patients with successful outcomes for the composite endpoints, preterm delivery and large for gestational age/ macrosomia have lower HbA1c levels than patients with poor outcomes, and this is evident throughout pregnancy.43 In our study Surinamese-Creole women had a significantly higher HbA1c value in trimester 3 compared with the other ethnic groups; however they did not show a higher birth weight, macrosomia or prematurity compared with other ethnicities. Since there were many missing data, no definitive conclusion can be drawn. According to a study from the USA, there is only limited evidence of an increased risk of large for gestational age/macrosomia among women with an HbA1c from 44 to 96 mmol/mol at diagnosis.44 The HbA1c ≥ 41 mmol/mol identified all women with diabetes and a group at significantly increased risk of adverse pregnancy outcomes according to a recent study from New Zealand.45 But not only should the HbA1c be maintained at a low level throughout pregnancy, also glucose profiles should be kept stable and high peaks of glucose should be avoided. Different studies support the association of hyperglycaemia with increased maternal, foetal and perinatal morbidity.32,35 In a randomised clinical trial, treatment of women with GDM, including dietary advice, blood glucose monitoring and insulin therapy, reduced the rate of serious perinatal outcomes (defined here as death, shoulder dystocia, bone fracture or nerve palsy) from 4% to 1% and a lower birth weight.46
CONCLUSIONS
In conclusion, in contrast to our hypothesis we did not find significant differences in neonatal complications between the six ethnicities. However, there are significant disparities in women with GDM in (percentile) birth weight and mode of delivery across different ethnic groups.
DISCLOSURES
We have no conflicts of interest to report.
REFERENCES
BIBLIOGRAPHY