KEYWORDS
Hypernatraemia, water-electrolyte imbalance, hospitalisation, prevalence, risk factors, prognosis
INTRODUCTION
Body water imbalance is common in hospitalised patients. Hyponatraemia reflects intracellular hyperhydration and occurs in up to one-third of patients; its causes and prognostic value are well established.1,2 Hypernatraemia is less common and less studied. It is nonetheless recognised as an important clinical condition, indicating a hyperosmolar state caused by a decrease in total body water relative to the electrolyte content, leading to intracellular dehydration. During the 2003 heatwave in France, intracellular dehydration was more common than intracellular hyperhydration (10.4% vs 8.0%) in older hospitalised patients, and predicted higher in-hospital mortality (hazard ratio 1.3 for intracellular dehydration compared with normohydration vs 1.1 for intracellular hyperhydration compared with normohydration).3 Although intracellular dehydration became less prevalent than intracellular hyperhydration (7.2% vs 9.5%) in the following years in the same settings, it was still associated with a higher risk of in-hospital death (hazard ratio 2.0 vs 1.3). Hypernatraemia has been associated with up to 60% inpatient mortality,4,5 but few studies describe risk factors, clinical profile and outcomes of patients with hypernatraemia in non-intensive care settings. The aim of the present study was therefore to evaluate the prevalence, risk factors and prognostic value of hypernatraemia in patients acutely hospitalised in an internal medicine department.
PATIENTS AND METHODS
Patients
Patients hospitalised in a 36-bed internal medicine department from January 2010 to May 2012 were retrospectively identified through the administrative database. Those with at least one plasma sodium ≥ 150 mmol/l (indirect potentiometry, Architect ci8200, Abbott Diagnostics, Rungis, France) during their stay were identified through the laboratory results database. Each hypernatraemic patient was individually matched for sex and age (± 1 year) with one patient hospitalised during the same period in the same department but who always remained normonatraemic (plasma sodium between 135 and 145 mmol/l).
Data collection and definitions
Data were collected, as appropriate, through the administrative and laboratory databases or chart review. Age, sex, chronic diseases, and functional ability were recorded for each patient. The Charlson index was used as a summary measure of comorbidities.6 We also considered the following data at admission: body temperature > 38°C, presence of oedema, systolic blood pressure (SBP), heart rate (HR), shock index (defined as the HR:SBP ratio), ongoing diuretic treatment, and estimated glomerular filtration rate (eGFR) according to the CKD-EPI equation.7 Main diagnosis, inpatient death and length of stay were recorded at the end of the stay.
Increased extracellular fluid volume was defined by the presence of oedema. Patients were defined as bedridden if they stayed in their bed to eat, to be washed and to pass stools. Patients were defined as autonomous for meals if they were able to ask for food and beverages and to eat and drink items within their reach without help.
Statistical analysis
The study period was determined by the possibility to retrieve and match biological and administrative data from hospital databases rather than by a formal sample size calculation. We first compared the sex and age of patients with at least one plasma sodium ≥ 150 mmol/l during their stay with all other patients. We then compared characteristics at presentation and outcomes of patients with at least one plasma sodium ≥ 150 mmol/l and matched controls who remained normonatraemic during their stay.
Descriptive statistics are reported as median [interquartile range] for continuous data and number (percentage) for categorical data. Differences were tested by the Mann-Whitney and the Fisher’s exact test, respectively, for unpaired comparisons, and by the Wilcoxon signed-rank or McNemar test for paired comparisons. Interaction tests were carried out with conditional logistic regression to check for a subgroup effect (pre-existing vs acquired hypernatraemia) on length of stay and in-hospital mortality. Differences were considered statistically significant if p < 0.05. All statistical analyses were performed with Stata 9.2 (StataCorp, College Station, Texas).
RESULTS
Plasma sodium was ≥ 150 mmol/l at least once during 49 of 1945 stays (hypernatraemia, 2.6%) and remained between 135 and 145 mmol/l during 1237 of 1945 stays (normonatraemia, 64%). Hypernatraemia was present at admission in 19 (39%) patients and was acquired during hospitalisation in 30 (61%). Median plasma sodium was 152 mmol/l at diagnosis of hypernatraemia in both subgroups.
Overall, hypernatraemic patients were significantly older than normonatraemic patients, without gender difference (table 1). Hypernatraemic patients and age- and sex-matched controls were similar in terms of Charlson index and vital signs at admission (table 1). However, they differed in the prevalence of several comorbidities included in the Charlson index, most notably heart failure and history of myocardial infarction (table 1).
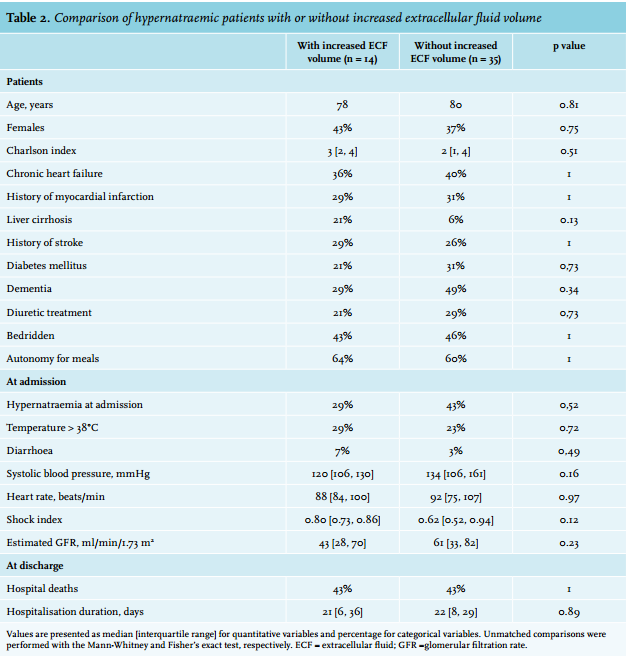
The shock index was higher and eGFR was lower in patients with hypernatraemia than in matched controls (table 1). Nearly one-third of hypernatraemic patients had increased extracellular fluid volume, ascertained by the presence of oedema (table 2). The underlying condition was heart failure in 36%, cirrhosis in 21% and hypoalbuminaemia of various mechanisms in 29%.
Main diagnoses were heterogeneous in both groups. The most frequent diagnoses were (i) acute respiratory events, mainly pneumonia and chronic obstructive pulmonary disease exacerbation (27% in hypernatraemic and 29% in normonatraemic patients, p = 1.00); (ii) acute neurological events, mainly delirium and stroke (33% in hypernatraemic and 14% in normonatraemic patients, p = 0.05).
Hypernatraemia was associated with much higher in-hospital mortality (43% vs 2%, p < 0.001) and length of stays that were twice as long (table 1). The interaction test revealed significant heterogeneity between pre-existent (at admission) or hospital-acquired hypernatraemia regarding the association with length of stay (p = 0.03) but not in-hospital mortality (table 1). 
DISCUSSION
Summary of results
About 3% of patients in a general internal medicine ward have hypernatraemia at admission or develop it during hospitalisation. They are older than other patients. Compared with sex- and age-matched normonatraemic controls, they have a similar number of significant comorbidities but of a different nature and with different functional consequences. Namely, they are more likely to have heart disease, to be bedridden and to depend on help for water intake. Hypernatraemic patients also have higher in-hospital mortality and longer hospital stays, especially when hypernatraemia is already present at admission.
Comparison with previous studies and interpretation
The frequency of hypernatraemia found in our study concurs with figures reported in previous studies, ranging from < 1% to > 3%.5,8-10 This wide variability in the frequency of hypernatraemia might be related to differences in the threshold used to define hypernatraemia, in the timing of hypernatraemia (at admission and/ or hospital-acquired) or in the study population. We defined hypernatraemia by at least one plasma sodium ≥ 150 mmol/l during hospitalisation, regardless of its timing but excluding patients with moderate hypernatraemia from 145 to 150 mmol/l. Moreover, we only included patients in the internal medicine department of our hospital. Only a few studies have focused on the same population. Most of the published papers relate to ICU or emergency room patients. One study performed in an internal medicine clinic showed an overall prevalence of 1.2%: 0.5% for hypernatraemia at admission and 0.7% for hospital-acquired hyponatraemia.5
We saw no gender difference between hypernatraemic and normonatraemic patients. This question has been controversial, as some studies found female gender to be a risk factor11,12 but others did not.13,14 On the other hand, our study confirms that age is a risk factor for hypernatraemia. One study dedicated to this question showed age as a strong independent risk factor.13 Thirst, a very important defence mechanism against hypernatraemia, is often disturbed in elderly patients. Moreover, elderly patients may have insufficient access to free water or difficulty to express thirst.11 This is consistent with our finding that hypernatraemic patients were more often bedridden and dependent on help for drinking. A recent study, focused on these questions, showed that patients admitted to hospital from care homes, who were more dependent or needed assistance for drinking, are frequently dehydrated and hypernatraemic at admission, and that these disorders are associated with higher in-hospital mortality.15
Unexpectedly, we found no significant difference in the Charlson comorbidity index between hypernatraemic and normonatraemic patients. However, a single summary score can be associated with many combinations of different comorbidities, and with different severity and functional impairment for each one. Myocardial infarction and chronic heart failure were the most frequent comorbidities found in the hypernatraemic group of our study. An association between hypernatraemia and a poorer prognosis in heart failure, independent of left ventricular ejection fraction, has been previously reported.16 Febrile illnesses, uncontrolled diabetes and gastrointestinal losses as diarrhoea were found to be risk factors for hypernatraemia in different studies,2,5,17-19 but we did not observe those associations in our work. Moreover, hypernatraemia is often associated with diuretic treatment, especially loop diuretics,2,5,16-20 but this was also not the case in our study.
A high shock index and low glomerular filtration rate are consistent with a lower effective arterial blood volume (true or effective hypovolaemia) in patients with hypernatraemia. According to textbook teaching, hypernatraemia is usually due to net water loss and associated with extracellular fluid volume depletion and true hypovolaemia.21,22 However, nearly one-third of the hypernatraemic patients in our study had oedema, indicating increased extracellular fluid volume. Still, according to textbook teaching, the few cases of hypernatraemia with increased extracellular fluid volume are due to excess intake of hyperosmolar fluids.22 This may well be the case in ICU settings, where hypernatraemia with increased extracellular fluid has already been documented,23,24 but not in our patients, who had classical causes of oedema such as heart failure, cirrhosis or hypoalbuminaemia. Impaired urinary concentrating mechanisms and reduced or hypertonic fluid intake compared with urine osmolarity are nonetheless necessary to generate hypernatraemia.25 Our hypernatraemic patients with a chronically increased extracellular fluid volume had an acute condition that led to decreased water intake or increased hypotonic losses leading to hypernatraemia before normalisation of their extracellular fluid volume. A more frequent use of loop diuretics may contribute to inappropriate free water clearance in patients with increased extracellular fluid volume, although this was not apparent in our study
The association of hypernatraemia with higher mortality has been previously reported in other populations: surgical patients,26,27 ICU patients,14,28-30 and heart failure patients.16 Mortality has been more frequently associated with hospital-acquired hypernatraemia despite the fact that these patients had a lower peak plasma sodium concentration than those who were hypernatraemic at admission.5,8-10,31 Acquired hypernatraemia in these patients may indicate less conscientious overall care, which could contribute to poorer outcomes.
However, it is important to stress that most previous studies were performed over 15 years ago and that the epidemiology and management of hypernatraemia has changed over time. Hypernatraemia is associated with serious underlying diseases, making it difficult to clarify the impact of hypernatraemia itself on the adverse outcome, especially if we consider that many hypernatraemic patients, whether at admission or acquired in hospital, were again normonatraemic before they died.5
Limits and strengths
Our study is limited by its retrospective and monocentric design and the small population analysed. Retrospectively collecting the clinical data of all normonatraemic patients was beyond our resources. However, matching is a powerful and hypothesis-free means to control for important confounding factors, such as age in our case. The comparison of hypernatraemic patients with or without increased extracellular fluid volume especially lacks power and we may have been unable to identify true differences between these subgroups.
Although the Charlson comorbidity index is validated and commonly used, this aggregated score masks different levels of severity for each disease and different patterns of association between them. Several substances and procedures that might influence serum electrolytes such as parenteral fluids and tube feeding were not considered. Parenteral fluids are likely to play a role in preventing hospital-acquired hypernatraemia, but we could not retrospectively retrace the data on administrated fluids, especially those used as a vehicle for parenteral medications. This study, like many others, cannot separate the contribution of hypernatraemia itself to mortality from that of the underlying frailty and acute condition.30 The present results can therefore not predict the impact of hypernatraemia correction on outcomes.
Nevertheless, our study has several strengths. Most published evidence on hypernatraemia in hospitals is over 10 years old and relates to intensive care units. Patients and management in our study are representative of contemporary in-patient recruitment and of current practices in a general internal medicine department. The matched design allows to control for age, the most important risk factor of hypernatraemia, and to look for independent risk factors. Comorbidities, functional status and extracellular fluid volume were taken into account.
Perspectives
The present study confirmed that elderly and dependent people are at risk to develop hypernatraemia, a condition associated with a poor prognosis. These results underscore that healthcare professionals and other caregivers need to increase their awareness and pay close attention to preventing water imbalance in home-cared and hospitalised elderly patients.12,19 The retrospective review of our patient records showed that administrated parenteral fluids are not appropriately traced, especially those used as a vehicle for parenteral medications, which is left to the nurses’ choice (in France). In many patients, these fluids add up to a large volume with possible clinical consequences in patients with or at risk of water and/ or sodium imbalance. The rational choice of these fluids and their prescription by physicians is an area for practice improvement.
When it comes to the consequences for clinical research, an evaluation of interventions to lessen the risk of hypernatraemia in at-risk patients may contribute to identifying the best preventive strategies. Moreover, as referred to before, the contribution of hypernatraemia itself to mortality cannot be separated from that of the underlying frailty and acute condition. The impact of hypernatraemia correction on prognosis needs to be assessed by interventional studies.
CONCLUSION
Hypernatraemia is more likely to occur in dependent patients, but with no more comorbidities than others. Unlike classical teaching, it is often associated with increased extracellular fluid volume even in non-ICU settings, due to heart failure, liver cirrhosis or hypoalbuminaemia of various causes. Hypernatraemia is a powerful risk factor for hospital death and longer hospitalisations, especially when it is present at admission.
DISCLOSURES
The authors have no conflict of interest to disclose.
REFERENCES