KEYWORDS
Epstein-Barr virus (EBV), mimicking lymphoma, T-cell non-Hodgkin’s lymphoma NOS
INTRODUCTION
Non-Hodgkin’s lymphoma is rarely associated with a previous Epstein-Barr virus (EBV) infection; however, EBV infection may also mimic non-Hodgkin’s lymphoma. We present a patient with an unusual course of EBV infection which was initially diagnosed as a T-cell non-Hodgkin’s lymphoma.
CASE REPORT
A 50-year-old male, without relevant medical history, presented to the emergency department with intermittent fever, muscle pain and fatigue for four weeks. Localising symptoms or other B-symptoms, except for fever, were absent. At presentation he was afebrile and physical examination was unremarkable and negative for lymphadenopathy or organomegaly. Laboratory investigations revealed the following: C-reactive protein 3 mg/l (< 10), leukocytes 19.4 x 109/l (4.5-11), leukocyte differential count showed bands 2% (0-5), segments 7% (45-75), lymphocytes 85% (20-50), monocytes 4% (2-10), basophils 2% (0-2) and many atypical lymphocytes, direct bilirubin 12 µmol/l (< 17), alkaline phosphatase 256 U/l (< 90), gamma-GT 665 U/l (< 50), aspartate aminotransferase 78 U/l (< 35), alanine aminotransferase 102 U/l (< 45), and lactate dehydrogenase 1241 U/l (< 248). Electrolytes and creatinine were normal. Urinalysis was normal and the chest X-ray showed no infiltrative abnormalities. Virus serology was negative for an acute infection with EBV (VIDAS Biomerieux: EBV IgM negative, EBV nuclear antigen (EBNA) negative, viral capsid antigen (VCA) IgG indeterminate), cytomegalovirus, hepatitis B, C and human immunodeficiency virus. Blood and urine cultures remained negative. Additional imaging was performed, computed tomography of the neck/ thorax/ abdomen showed cervical (7 and 12 mm), axillary (8 and 11 mm), mediastinal and hilar (12 mm) lymphadenopathy and splenomegaly (15 cm). Additional diagnostic lymph node extirpation and bone marrow biopsy were performed.
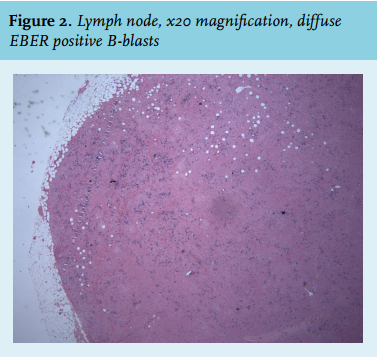
The lymph node revealed disturbed architecture and expansion into the adjacent tissue. The paracortical expansion is caused by an increase in T-lymphocytes (figure 1), resulting in a strong suspicion of a peripheral T-cell non-Hodgkin’s lymphoma not otherwise specified (NOS). Clonality analysis confirmed monoclonality of the T-cell population. Immunohistochemistry revealed a T-cell fraction which shows a uniform and strong immunoreactivity with antibodies against Ki67 and in the background Epstein-Barr virus-encoded small RNA (EBER) positive blasts (figure 2). Bone marrow biopsy also revealed a peripheral T-cell non-Hodgkin’s lymphoma NOS. Morphological analysis showed a strongly increased lymphopoiesis of 54% and at immunophenotyping 47% were lymphocytes of which 41% T-lymphocytes, especially CD8+. Clonality analysis of the lymph node and bone marrow showed an identical clonal T-cell population.
In conclusion, our patient was diagnosed with a stage IV T-cell non-Hodgkin’s lymphoma NOS. Suggested treatment was two weekly cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP) chemotherapy followed by autologous stem cell transplantation. At presentation to the outpatient clinic he was asymptomatic and the laboratory results had normalised. Virus serology was repeated on serum drawn seven days after the first serology was performed, as a biomarker of a T-cell non-Hodgkin’s lymphoma; this test was positive for EBV with VCA IgG and IgM and the EBNA test was positive (Diasorin LIAISON® EBV). The first serum sample was tested for EBV DNA by polymerase chain reaction (PCR), the result was positive 3.9 x 104 copies/ml. Chemotherapy was cancelled. CT scan was repeated and showed no lymphadenopathy and a normalised spleen volume. EBV PCR was dubiously positive after one month and one year of follow-up. Follow-up bone marrow analysis after three months and one year revealed an unchanged identical clonality analysis but a decreasing abnormal T-cell population (41%, 39% and 11% respectively). Eventually this was diagnosed as an unusual course of EBV infection, after the initial diagnosis of T-cell non-Hodgkin’s lymphoma. The clinical relevance of the remaining small monoclonal T-cell population detectable in the bone marrow is unclear.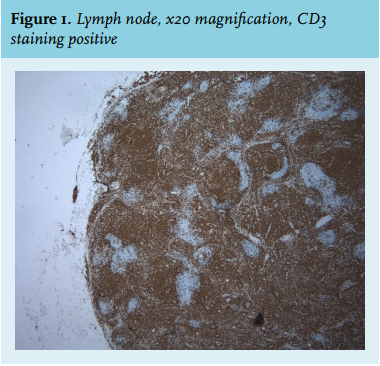
DISCUSSION
Epstein-Barr virus is a widespread herpesvirus and the primary agent of mononucleosis infectiosa. An IgM class antibody directed against the viral capsid antigen (anti-VCA IgM) is the first humoral response. In one article Odumade et al. reported that 90% of the anti-VCA IgM became positive within seven days of onset of symptoms, in six patients they became positive during the second week of illness and one did not become positive until 49 days after onset of illness. Anti-VCA IgG antibodies were developed in all patients, which peak during the first two to four months and then persist during life. Those antibodies may present in acute infection but in smaller quantities than anti-VCA IgM.1 Circulating cell-free EBV DNA has been detected in plasma/ serum from patients with EBV-associated tumours.2 In approximately 40% of peripheral T-cell lymphomas NOS EBV is detected. There is an association between EBV infection and the development of Burkitt’s lymphoma, nasopharyngeal carcinoma, Hodgkin’s lymphoma and in very rare cases of natural killer cell T-cell lymphomas. The exact mechanism is as yet unclear.3 Additionally, it has been described in the literature that morphological characteristics of an EBV-infected lymph node can imitate a lymphoma. One case series was published which describes 18 cases with acute EBV infection, all of which were suspicious for or initially diagnosed as a malignant lymphoma.4
CONCLUSION
Acute EBV infection may present in different ways and can mimic malignant lymphoma at presentation. Negative EBV serology can be misleading. We advise an EBV PCR in case of a clinical suspicion of EBV infection or confirmation by a different serological test. When a spontaneous clinical improvement occurs in a patient diagnosed with a lymphoma, an extreme course of EBV infection must be considered.
DISCLOSURES
No conflict of interest.
REFERENCES