KEYWORDS
Four hour target, completion times, academic hospital, peripheral hospital
INTRODUCTION
Long completion time in the emergency department (ED) can lead to overcrowding and is associated with negative outcomes, such as increased risk of hospital admission and in-hospital mortality.1 Therefore, optimising ED patient flow is an important and frequently discussed topic. Because the frequency and type of presentations are unpredictable, it remains a challenge for emergency physicians and nurses to provide adequate care for all patients, especially during the busiest moments.
Overcrowding and long ED completion times can occur when the maximum available care does not meet increasing demands. A recent study demonstrated that visiting an ED on crowded days resulted in delays in resuscitation efforts and higher in-hospital mortality.1 Also in discharged patients, it has been noted that a long stay on the ED was associated with increased risk of hospital admission within seven days and mortality.2 In that light, we previously conducted a study at the VU University Medical Center, Amsterdam, the Netherlands (VUmc), to obtain insight into factors which could contribute to a completion time of more than four hours, and we demonstrated that a vast majority of the patients left the ED within four hours (84%).3 However, the patients exceeding the four hours were older, sicker and treated by multiple consulting specialists. In addition, after finishing all the diagnostic tests, there was a marked delay until discharge, probably caused by inefficient decision-making by the junior doctors.3 This study was conducted in a single academic centre only and therefore was not generalisable to community hospitals. For that reason, we decided to conduct a new study in two different hospitals: an academic centre and a large community hospital. The primary aim was to examine which factors currently contribute to overcrowding and completion times longer than four hours on the ED in the VUmc, a level 1 academic trauma centre and on an ED in a large community hospital, the St. Antonius Hospital in Nieuwegein, the Netherlands and whether or not these hospitals encounter the same problems in patient flow on the ED.
MATERIALS AND METHODS
Study design and setting
This prospective study was performed in the EDs of the VUmc and St. Antonius Hospital.
VUmc is an academic urban level 1 trauma centre in Amsterdam with approximately 29,000 ED visits per year. During the study period there were 11 residents in emergency medicine, including seven fellows of emergency medicine and four non-trainees working in shifts. Residents were supervised by four qualified emergency physicians (EPs) and one surgeon. The emergency medicine trainees and EPs belong to the surgical staff. At the ED of the VUmc, all patients presenting themselves without a referral from a general practitioner are seen by emergency medicine residents and qualified EPs. Depending on the needs of the patient, the EP can consult the medical specialists. If a patient needs more specialised care or needs to be admitted to the ward, the necessary specialism is consulted and the patient is handed over to the specialist for further treatment. Referred patients are seen by (non) trainee residents of various medical specialities under the supervision of medical specialists belonging to the particular department. St. Antonius Hospital is a large community medical centre with approximately 23,000 visits per year. There were seven trainee residents in emergency medicine working in shifts. Non-referred patients were seen by EP residents and supervised by qualified EPs and referred patients were seen by residents of a specific speciality supervised by the medical specialist. However, senior EPs were able to admit a patient for a specialism directly to the ward after a phone consultation with the specialist on call.
Selection of participants, data collection and processing
In the VUmc the study was conducted during a four-week period from 8 October until 4 November 2012. At St. Antonius Hospital, this was divided into two periods of two weeks each from 21 November until 5 December 2012, and from 11 February until 24 February 2013.
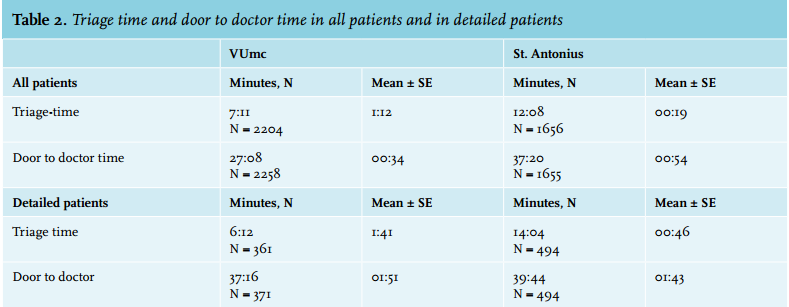
For all patients visiting the ED in these aforementioned weeks, the following time moments were registered: ED arrival, triage, first contact with a physician, and discharge from the ED, in addition to information on triage level, type of referral, ordering of radiological and diagnostic testing, discharge disposition, first and last consulting medical speciality and the total number of consultations. At VUmc, these data were extracted from paper forms filled in by nurses and physicians. At St. Antonius Hospital, data were retrieved from a computer system called Intracis.
In addition, data were collected by trained observers (medical students under the supervision of an internal medicine resident and a specialist) to obtain detailed information on different consecutive steps in the process of individual ED patient flow. The observers worked in shifts to cover all the days of the previously defined study periods, from 12.00-23.00 hours. For this additional follow-up, patients older than 18 and triaged to Emergency Severity Index (ESI) level 2 or 3 at VUmc, and Manchester Triage System (MTS) category orange or yellow at St. Antonius Hospital were selected.4,5 This selection was based on the previous measurement, demonstrating that these categories had longer completion times.3
The additional data collection included time moments for the ordering, conduction and evaluation of radiological and diagnostic testing and the request, conduction and ending of a medical consultation. Also data on the time physicians arrived at their final diagnostic conclusions on the ED and when the nurses were informed that the patient could leave the ED were noted.
Outcome measures
The primary aim of this study is to measure the durations of the different diagnostic and therapeutic procedures that a patient is subjected to during their stay in the ED, and to evaluate which factors contribute to completion times longer than four hours. Secondly to compare whether there are differences in completion times between an academic centre run by ED physicians and also fellows and specialists from various departments and a large urban hospital run primarily by the EPs. And thirdly/finally to investigate whether the measures implemented after previous measurement at the VUmc have had a beneficial effect on completion times.
Primary data analysis
Data from the VUmc and St. Antonius Hospital were analysed separately. Exceeding a completion time of four hours was selected as the primary endpoint. Patients were split into two groups: patients with a completion time on the ED of less than four hours or a completion time of more than four hours.
For statistical analyses, two types of statistical tests were used. Pearson’s chi-square test was used to assess the independence between the variable ‘exceeding or not exceeding the four-hour target’, and other variables including age category, triage level, and the number of consultations. The null hypothesis, which is an independence between the two variables, was rejected if the p-value was lower than 0.05 (significant dependency). The Mann-Whitney test, also called Wilcoxon or rank-sum test, was performed to compare the two populations of patients (exceeding and not exceeding the four-hour target) in terms of some duration variables. If the p-value was lower than 0.05, the null hypothesis that the distributions are similar was rejected, which means that the two distributions are significantly different and there is a significant dependency between exceeding / not exceeding the four-hour target and the chosen variable. The test allowed us to see whether the two populations had significantly different distributions of some durations such as door-to-doctor time and diagnostic tests for instance, and thus to know if there is a dependency between the two variables.
RESULTS
Characteristics of the study subjects
In the VUmc, 2272 patients were seen at the ED between 8 October and 4 November 2012, a total of four weeks. A subgroup of 372 ESI 2 and ESI 3 patients was followed closely by researchers to obtain more detailed information. In the St. Antonius Hospital there were 1656 patients of which a total of 492 orange- and yellow-triaged patients were closely observed for detailed information. The average age of patients in the VUmc was 40 years (SD 24.1); this was significantly higher in the St. Antonius Hospital with an average age of 50 years (SD 23.6), p < 0.001. Characteristics of all patients in both hospitals are summarised in table 1.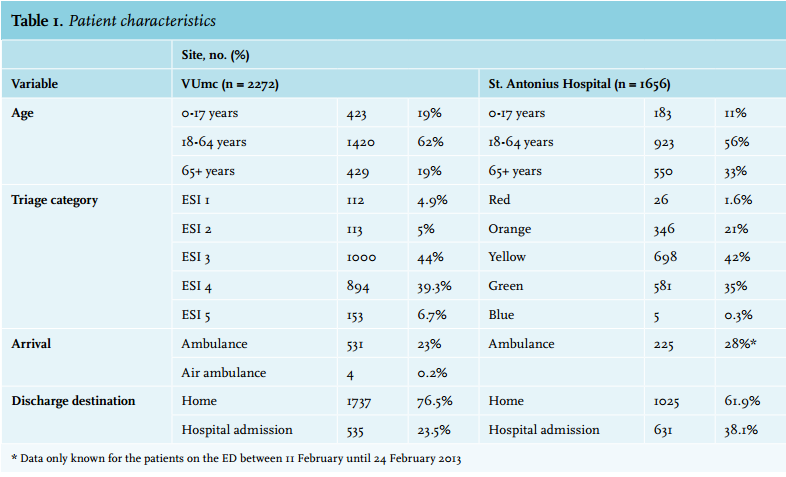
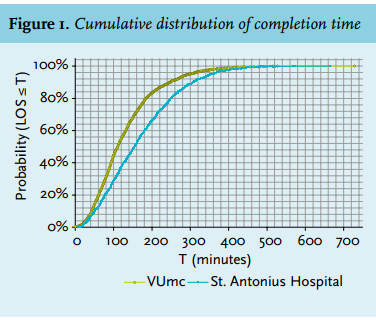
Time to completion
In the VUmc, 89% of the patients had a completion time of less than four hours. The average completion time (n = 2262) was 2:10 hours, (median 1:51 hours, range: 0:05-12:08). In the St. Antonius Hospital, 77% of patients had a completion time shorter than four hours (n = 1656). The average completion time in hours (n = 1655) was 2:49 (median 2:34, range: 0:08-11:04). Figure 1 demonstrates the cumulative distribution of completion times for both hospitals.
Triage In the VUmc, most patients were categorised as ESI 3 (44%) and ESI 4 (39%) (table 1). A larger percentage of ESI 1, 2 and 3 patients did not achieve the four-hour target (14%, 20% and 19%) compared with ESI 4 and 5 patients (2.7% and 0%), p < 0.001.
At the St. Antonius Hospital, most patients were categorised as yellow (42%) and green (35%). A greater percentage of orange and yellow categorised patients exceeded the four-hour target (32% and 28%) compared with red (8%) and green/blue (13%), p < 0.001.
Number of specialities involved
In the VUmc, the average number of consultations per patient was 1.306, this was 1.155 in St. Antonius. For both hospitals there was a significant dependency between exceeding the four-hour target and whether a consultation was performed (p < 0.001). The realisation of the four-hour target was not linked to the number of consultations.
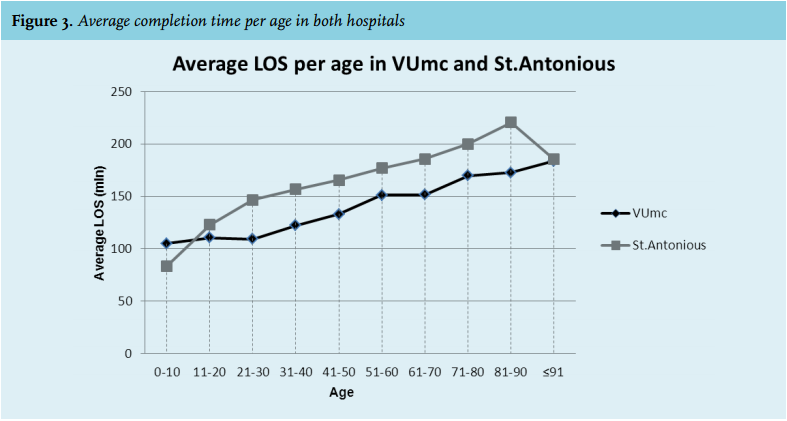
Age
In both hospitals, patients older than 65 years were more likely to stay in the ED for more than four hours (p < 0.001). Figure 3 demonstrates the average completion time per age category.
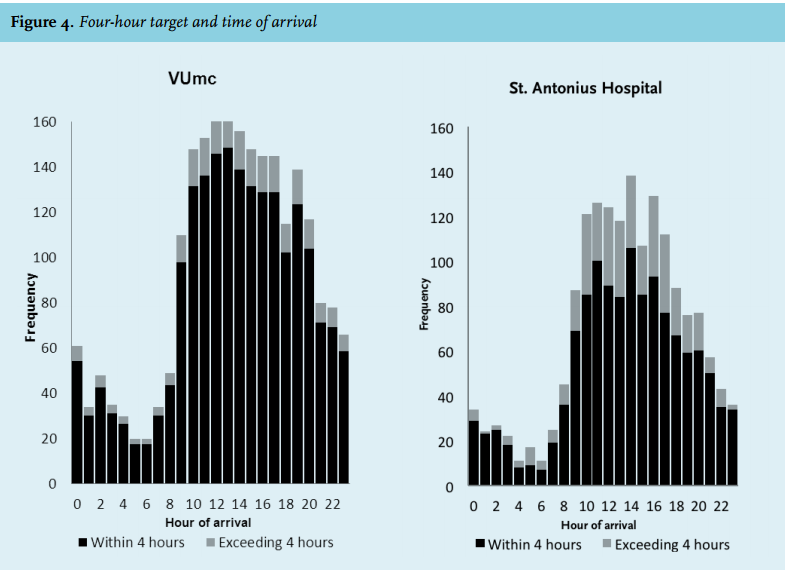
Arrival pattern
Most patients arrived between 9.00 and 23.00 hours. An association was found for both VUmc (p = 0.02) and St. Antonius Hospital (p = 0.02) between arrival time and the four-hour target (figure 4). No significant differences were found in exceeding the four-hour target between ED visits on different days of the week: VUmc (p = 0.054), St. Antonius Hospital (p = 0.16) 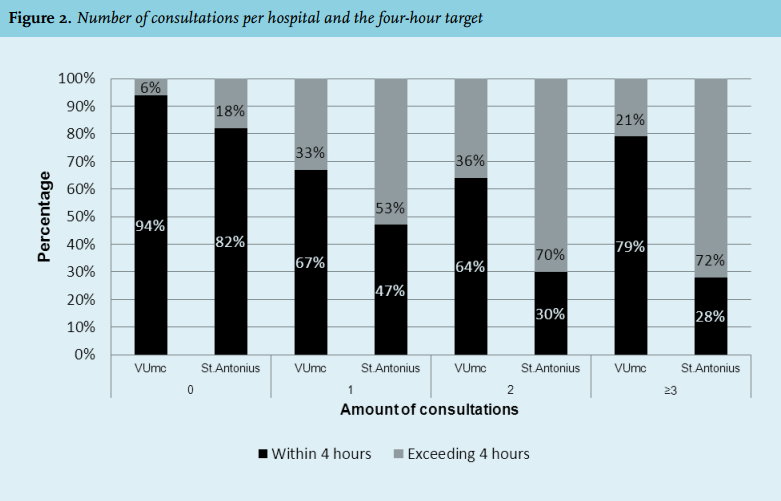
Door-to-doctor time
In the VUmc, the door-to-doctor time was not significantly different between patients who did or did not exceed the four-hour target, p = 0.07 (figure 5). In St. Antonius Hospital, there was a significant correlation for this analysis, p < 0.001 (figure 5). The door-to-doctor times for all patients and for detailed measured patients are demonstrated in table 2. 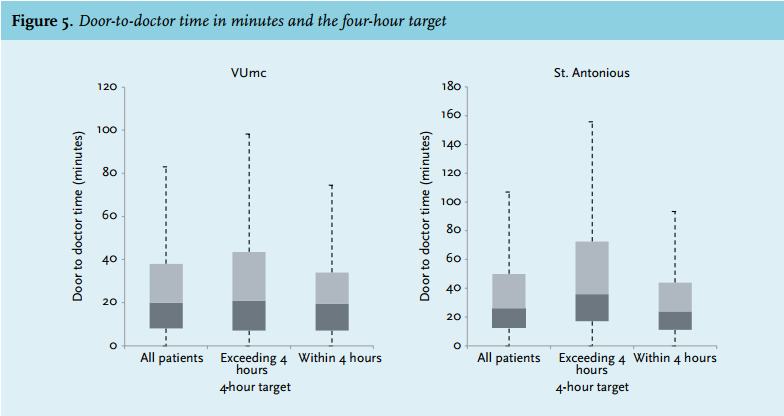
Medical speciality
In the VUmc, most patients were seen by EPs and 4% of these patients exceeded the four-hour target. In 29% of the surgery patients, the four-hour target was exceeded, followed by neurology (27%) and internal medicine (24%). In the St. Antonius Hospital, most patients were seen by the EPs on behalf of different departments. The internal medicine department had the largest percentage of patients exceeding the four-hour target (40%) followed by lung diseases (35%) neurology (33%) and surgery (14%). In both hospitals a significant dependency was found between speciality and exceeding the four-hour target (p < 0.001).
Diagnostic tests
In the VUmc data of 283 detailed patients were useful for analysing diagnostic tests, as illustrated in figure 6. No significant difference in duration of ‘prediagnostic tests’ was found for patients who did or did not exceed the four-hour target (p = 0.12). For ‘diagnostic tests’ and ‘time after diagnostic tests’ there was a significant difference (both p < 0.001). In the St. Antonius Hospital there was a significant difference in the duration of all the sub-processes for patients (n = 349) who did or did not exceed the 4 hour-target. 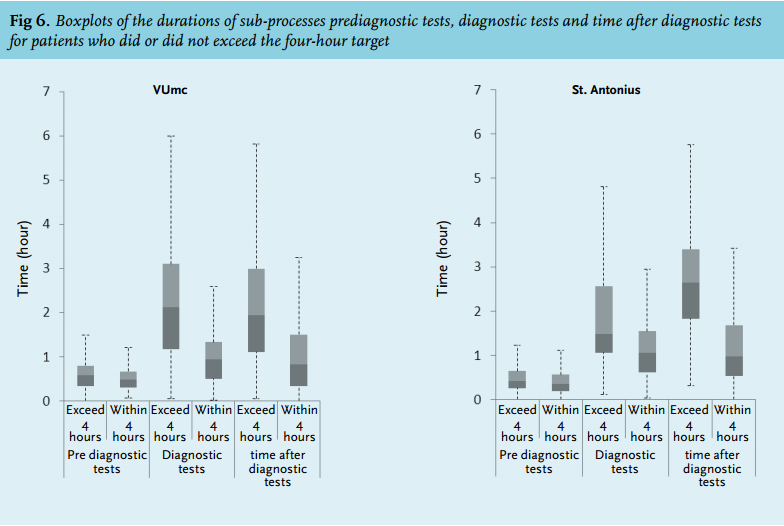
Radiology
In the VUmc, 34% of patients underwent an X-ray, followed by CT scan (11.4%), ultrasound (8%) and MRI (0.4%). In the St. Antonius Hospital, 49% of patients underwent an X-ray, followed by CT scan (15%), ultrasound (7.9%) and MRI (0.4%). All radiology tests were correlated with a significantly higher chance to exceed the four-hour target. The patients in the VUmc who did not undergo any radiological tests had a chance of 4.9% of exceeding the four-hour target. This chance to exceed the target increased to 8.5% in patients only undergoing X-ray(s) (p = 0.002), and to 35.3% for patients only undergoing CT scan(s) (p < 0.001) and 33.3% for patients undergoing only ultrasound(s) (p < 0.001). In the St. Antonius Hospital the chance to exceed the four-hour target was 11% for those who did not have radiological tests. This chance increased to 22% for patients having only X-rays(s) (p < 0.001), to 49% for patients undergoing only CT scan(s) (p < 0.001) and to 45% for only undergoing ultrasound(s) (p < 0.001). For both hospitals there was a significant correlation for the number of radiology tests and exceeding the four-hour target (p < 0.001), as shown in figure 7.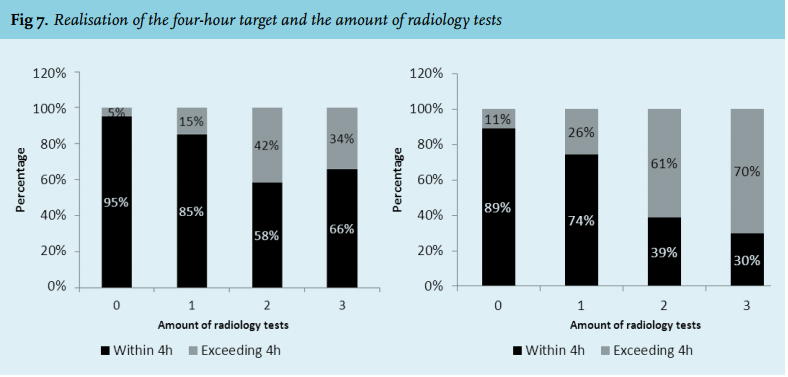
Discharge destination
In both hospitals, most ED visits did not result in a hospital admission (table 1). Patients who were admitted or transferred elsewhere were more likely to exceed the four-hour target in the VUmc (25% and 29% of exceeding) compared with those who were discharged (7%) (p < 0.001). In the St. Antonius Hospital 37.5% of admitted patients and 57.1% of transferred patients exceeded the four-hour target compared with 11.5% of released patients (p < 0.001).
VUmc 2010 compared with 2012
In February 2010, 84% of patients in the VUmc had a completion time of less than four hours and the average completion time was 2:23 hours (n = 2444). This was 89% in 2012 with an average completion time of 2:10 hours (n = 2262).
The average door-to-doctor time was 48 minutes in the subgroup of detail patients (n = 66) in the study of 2010. This was 37 minutes in the subgroup of 371 detail patients in this study in 2012.
In the previous study and in this study, no association was found in the VUmc between the arrival time of a patient and the four-hour target. The previous study in the VUmc demonstrated that internal medicine had most patients exceeding the four-hour target (37%), followed by neurology (29%) and surgery (28%). In this study, internal medicine accounted for 24% of the cases exceeding the four-hour target. In both studies, 39% of patients were triaged as ESI 3. In 2010, 24% of these patients did not achieve the four-hour target, this was 19% in 2012. In both studies the absolute number of patients exceeding the four-hour target, were ESI 3 patients. In 2010 and 2012 for both sub-process ‘diagnostic tests’ and ‘time after diagnostic test’ there was a significant difference in durations of patients who do and do not exceed the four-hour target.
DISCUSSION
In this study we found that patients older than 65 years, patients seen by more than one specialism and patients undergoing radiological tests are more likely to have longer completion times in both hospitals. We aimed to detect factors contributing to a longer stay on the ED in two hospitals with different work procedures and different patient populations. In the VUmc a higher percentage of ESI 1 patients were seen compared with the number of red-triaged patients in the St. Antonius Hospital, due to the fact that the VUmc is a level 1 trauma centre. However, more orange-triaged patients were seen in the St. Antonius Hospital compared with ESI 2 patients in the VUmc, probably because acute cardiology patients (mostly ESI 2) are not presented to the ED in the VUmc but to the cardiology department. Notably, more older patients were seen in the St. Antonius Hospital. In the VUmc, non-referred patients were seen by EP trainees who were supervised by a qualified EP. If the expertise of a specific speciality was needed, a resident of this speciality was consulted and supervised by the medical specialist. Referred patients were directly seen by the residents of a specific speciality and supervised by the medical specialist. In the St. Antonius Hospital, non-referred patients were mostly seen by EP residents and referred patients were mostly seen by residents from the speciality. However, in St. Antonius Hospital senior EPs were able to independently discharge or admit a patient for a specific speciality after a phone consultation with a medical specialist of the department. Probably as a result of this difference in work procedure, more consultations were performed in the VUmc.
Despite these differences, both hospitals were facing largely the same problems. Factors increasing the chance of exceeding the four-hour target were: older age, having at least one consultation and undergoing radiological testing. These patients were predominantly found in the higher triage categories. However, in the most acute category (ESI 1 or category red), patients are treated in the shock room by a team of specialists directly after arrival on the ED with the opportunity to perform radiological testing at the bedside, resulting in a relatively short completion time on the ED. Patients in triage categories ESI 2/3 and orange/yellow, however, are not initially seen by a team of specialists despite the fact that this group of patients is also relatively old and frequently have multiple comorbidities demanding the expertise of more than one specialist.
Consultations occurred consecutively in these patients contributing to a longer completion time in both hospitals. Brick et al. also concluded that multiple consultations and advanced age were significantly associated with a longer stay on the ED.6 Consulting physicians tend to treat the patient individually, one after the other, instead of working as a team. This fragmented delivery of care increases the length of stay and may thereby lead to complications and reduced patient satisfaction. A proposed solution for this problem in our previous study was the introduction of assessment teams for these patients. Especially in old patients with multiple comorbidities it was decided that specialities such as internal medicine, neurology, surgery or emergency physicians should be called upon to examine the patients together as a team at the outset so that multiple, consecutive consultations could be avoided. However, although we have propagated this concept intensively in the last few months the doctors still seem to follow the traditional method of examining/treating these patients consecutively one after the other.
In 2010, the completion times were measured in the VUmc in order to explore the delaying factors contributing to stagnation on the ED. After the results were known, new measures were implemented to improve the patient flow. The most important measure was that the supervising internist stayed in the hospital until 23.00 hrs. instead of 18.00 hrs. In addition the shifts covered by qualified EPs were adjusted. During weekdays the shifts were extended from 08.00-17.00 hrs to 08.00-23.00 hrs and in the weekend they were available for supervision by phone. Two years later we noticed some improvements, the completion time within four hours increased from 84% in 2010 to 89% in this study. The internal medicine department showed the largest decrease in patients exceeding the four-hour target, from 37% to 24%. This is probably due to the increased working hours of the supervising internist, which probably quickens the decision-making process. Bucheli also demonstrated that adding a second physician during the evening shifts of the internal medicine department significantly reduced the time spent on the ED.7 In addition the change in the mindset of the residents and specialists of the internal medicine department after the publication of the first results might have improved the working efficiency on the ED of this specialism.
Despite booking the above-mentioned improvements compared with 2010, we do experience some of the same problems in the VUmc. We still see patients stay relatively long on the ED after all the diagnostic tests are finished. After interviewing some of the nurses and residents, it was proposed that the main cause for this delay was the lack of direct supervision on the ED. Residents often see patients alone on the ED and telephone their supervisor after finishing anamnesis, physical examination and first diagnostic tests. They tend to collect patients and/ or problems before they call their supervisor, especially during late hours when the senior specialist is no longer in the hospital. In addition, during the daytime supervisors are not always directly available to discuss a case on the phone with the resident, because they are also busy supervising on the wards or the operating room.
Furthermore, the use of diagnostic procedures such as CT scans has increased in the last decade, as they improve diagnostics and therapeutic decision-making, but on the other hand they also take up a long completion time.8,9 In this study, all radiological tests were correlated with a longer completion time on the ED, and CT scan especially. It is known that it takes time before all the images of the CT scan are uploaded and available for the radiologist to interpret. In our opinion more emphasis should be placed on timely performance and interpretation of radiology testing in the ED setting.
Even though ED crowding and long completion times are an intensely debated issue and a serious problem in many countries, the Netherlands together with some other Scandinavian countries seem to perform relatively well in delivering timely patient care at the ED.10 This may also be due to a strong network of patient care outside the ED, such as the prehospital and primary care that is also available after-hours, which makes it easy for the clinicians to discuss the case with GPs and take necessary measures together. However, the patients who do stay longer in our hospital are old and vulnerable, which increases the risk of complications in this group. As shown in an earlier study these patients are known to have about three comorbidities and used an average of 5.3 different medications.11 Therefore, in our opinion these results should be taken seriously and remedial measures such as introduction of assessment teams, improving the direct supervision of the resident to speed up the process of decision-making, and increasing the radiological support in the ED should be introduced in the EDs.
This study was performed in two large hospitals with a large number of inclusions which makes the conclusions generalisable to the situation in the Netherlands.
STUDY LIMITATIONS
Firstly, in this study detailed information was only obtained by the researchers for ESI 2/3 and orange/yellow categorised patients. We chose to closely observe this group because earlier research pointed out that this group had, in absolute numbers, the longest completion time on the ED. Selection of these patients might underexpose logistic problems occurring in the other triage categories. However, as the completion time in these triage categories was significantly lower we presume the impact of this selection on the overall results was minimal.
Secondly, the triage systems of hospitals were different, which can introduce bias. However, in the Netherlands both triage systems are frequently used and are largely comparable in determining the severity of the condition of the patient.
Thirdly, the measuring period was not at the same time in the two hospitals. Seasonal influence may alter the situation. However, the benefit of measuring in both hospitals one after another is that we had the same team of researchers, using the same technique during both study periods. Finally the researchers were physically present on the ED floor to note every step in the process of the selected patients. This might alter the attitude of the treating physician/nurses, and speed up or slow down the normal routine of the physicians and nurses on the ED.
CONCLUSION
In this study performed on the EDs of two different hospitals with different working strategies and patient populations, we see that the factors leading to ED stagnation were similar, namely: old age of the patients, treatment by more than one speciality and undergoing radiological tests. Compared with the measurements in 2009 for the internal medicine department, we do see some improvements in the VUmc during this study. This department extended the hours in which the supervising specialist was in the hospital after the study results in 2009. This more direct contact between supervisors and residents might help to quicken the process of decisionmaking, after all diagnostic tests are performed. Despite this small improvement, still the same vulnerable group of patients has the longest completion time on the ED. We noticed that it is difficult to make substantial changes in the workflow of an emergency department. We still think that uniform remedial measures should be taken nationwide to deal with these factors to reduce stagnation in the EDs.
DISCLOSURES
The authors declare no conflicts of interest.
REFERENCES