KEYWORDS
Cardiovascular risk, primary prevention, secondary prevention, statins, undertreatment, underuse, risk assessment
INTRODUCTION
In the early 1990s, several landmark trials unequivocally showed that HMG-CoA reductase inhibitors, i.e. statins, reduce cardiovascular morbidity and mortality in secondary as well as primary prevention through lowering low-density lipoprotein cholesterol (LDL-c) levels.1,2
There are to date only very few reports on the use of statins for primary prevention. Data from the Oslo Health Study (collected in 2000-2001) showed that most participants with diabetes were not treated, especially women.3 In 2003, it was shown that over 95% of the population eligible for pharmacological treatment of hypercholesterolaemia were untreated or uncontrolled in a Dutch population-based cohort study.4 It was subsequently shown that the use of cardiovascular drugs increased over time in the Netherlands,5 but recent figures on the implementation of cardiovascular disease (CVD) guidelines for the use of lipid-lowering drugs (LLD) for primary and secondary prevention are lacking. The need for continuous awareness was recently illustrated by the observation in the USA that only 20% of individuals with a ten-year CVD risk > 20% were treated with statins.6
For patients who suffered from CVD (secondary prevention), several studies in the late 1990s highlighted that undertreatment was also common.7 In a representative survey of the US population, it was recently shown that only 58% of patients with coronary artery disease were treated with statins.8
The general aim of guidelines is to assist physicians in selecting the best treatment strategy for an individual patient. The indication to prescribe LLD in the Netherlands is based on the national CardioVascular Risk Management (CVRM), written by the Dutch Institute of Health Care Improvement and the Dutch College of General Practitioners (NHG).9 Concerning primary prevention, the Dutch CVRM uses dedicated prediction charts, based on Dutch prospective cohort studies, to calculate the ten-year risk of cardiovascular morbidity or mortality (ten-year CVD risk). This ten-year CVD risk is stratified as low (< 10%), medium (10-19%), or high (≥ 20%) risk. Patients at high risk with LDL-c levels > 2.5 mmol/l and patients with a total cholesterol/high-density lipoprotein cholesterol (TC/ HDL-c) ratio > 8 are all eligible for LLD prescription. LLD treatment is only recommended for patients at medium risk when they present with LDL-c levels > 2.5 mmol/l and one or more additional risk factors (sedentary lifestyle, positive family history of premature CVD, obesity and renal failure). Concerning secondary prevention, patients with myocardial infarction and those who have undergone coronary surgery should be treated. The same holds true for those who have suffered from stroke or peripheral vascular disease and have LDL-c levels > 2.5 mmol/l (table 1).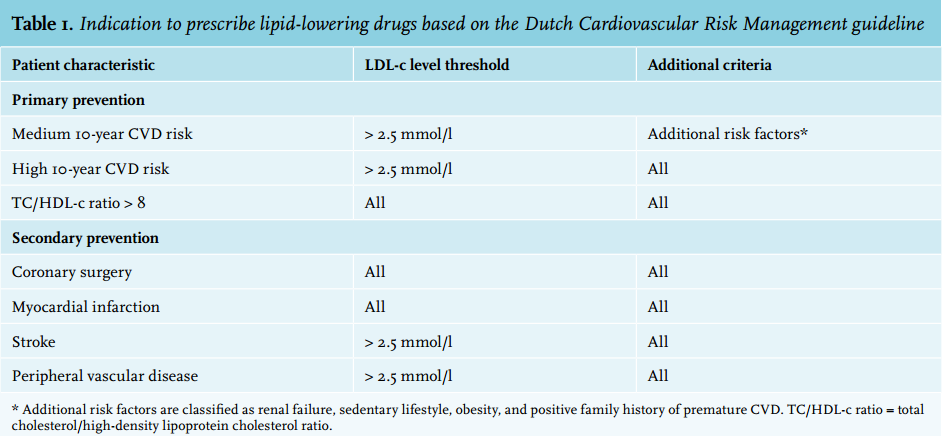
International guidelines were recently compared by Saraf et al. 10 Overall, the Dutch guidelines are quite similar to the international guidelines; however, there are some differences. While most international guidelines recommend statin treatment if LDL-c levels are ≥ 4.9 mmol/l, the Dutch CVRM does not include this. The CVRM guideline is unique in its recommendation for treatment in patients with a medium ten-year CVD risk in combination with additional risk factors.
To tackle undertreatment, the NHG is dedicated to improving implementation of these guidelines through developing e-learning modules, organising courses, and generating protocols for nurse practitioners, brochures and websites for patients. The Dutch Heart Foundation has also developed standards for managing cardiovascular risk factors to improve implementation. To improve the awareness of cardiovascular risk in the general population a National Cholesterol test was initiated in 2014.
In the current study, we evaluated the use of LLD in both primary and secondary prevention in a large sample of the Dutch general population (LifeLines study).
METHODS
Study design and participants
LifeLines is an observational population-based study of the Northern provinces of the Netherlands.11 The study protocol was approved by the medical ethics committee of the University Medical Centre Groningen. All participants provided written informed consent.
For the current study, baseline data were available of 70,292 participants who were recruited between 2006 and 2012. Participants were excluded if data to calculate the ten-year CVD risk were missing or when medication use was not verified. Individuals who reported a myocardial infarction, stroke, or coronary revascularisation procedures, defined as coronary angioplasty or bypass, were classified as secondary prevention. The remainder were classified as primary prevention. Peripheral vascular disease was not addressed in the LifeLines questionnaires and could unfortunately not be evaluated.
Questionnaires and physical examination
Baseline questionnaires included questions on demographics, family structure, medical history, lifestyle factors and medication use. For the current study, statins and ezetimibe were grouped as LLD. The use of fibrates was not taken into consideration for the current study because fibrates are not the first-choice treatment to lower LDL-c levels. All participants visited the LifeLines research site for physical examination, which included measurement of blood pressure (ten times using an automated blood pressure monitor; Dinamap), body height and weight. Hypertension was defined as systolic or diastolic blood pressure higher than 140 or 90 mmHg, respectively. Positive family history was defined as a parent or sibling who suffered from premature CVD (before the age of 50 years). Sedentary lifestyle was defined as less than 30 minutes of physical activity a day. Estimated glomerular filtration rate (eGFR) was determined using the Cockcroft-Gault formula. Fasting blood samples were collected. Total cholesterol and LDL-c levels were measured with a direct assay (Roche Modular P, Mannheim, Germany). High-density lipoprotein cholesterol (HDL-c) was measured via a direct quantitative assay (Roche Modular P, Mannheim, Germany). Triglycerides were measured using an enzymatic colorimetric test (Roche Modular P, Mannheim, Germany).
Recommendation for treatment and assessment of CVD risk
The CVRM guideline was used to decide whether or not participants were eligible for using LLD. The ten-year risk of cardiovascular morbidity or mortality of each participant was calculated using a risk prediction score according to the CVRM guideline.9 This algorithm used gender, age, smoking status, systolic blood pressure and TC/HDL-c ratio as the main risk determinants. The risk of participants with rheumatoid arthritis and diabetes mellitus was calculated by adding 15 years to the actual age.9 The ten-year risk of cardiovascular morbidity or mortality was stratified as low (< 10%), medium (10-19%), or high (≥ 20%) risk.
Statistical analyses
For statistical analysis PASW Statistics (Version 20, IBM, Armonk, NY, USA) was used. Participants’ baseline characteristics were presented by mean, standard deviation (SD) and ranges or by percentages in case of categorical variables. We assessed which individuals should receive LLD according to the CVRM guideline. Recommended treatment was compared with the self-reported treatment.
For both primary and secondary prevention, differences between those reporting and not reporting LLD treatment were compared using a Student’s t test or Mann-Whitney U test. We further explored undertreatment in different subgroups. All statistically significant subgroups in univariate logistic regression (data not shown) were assessed in subsequent multivariate logistic regression, adjusted for sex and age, to analyse independent predictors of not reporting LLD.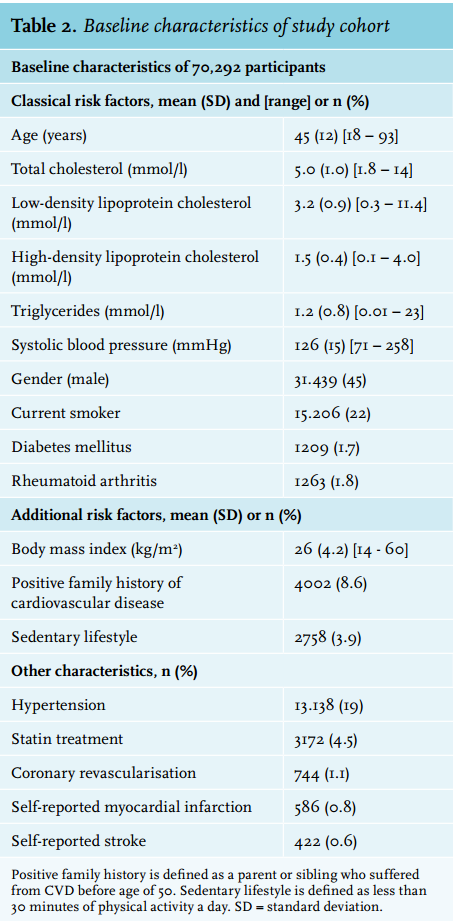
RESULTS
Baseline characteristics of study cohort
The study population consisted of 70,292 participants. Baseline characteristics are shown in table 2. Briefly, themean age of the participants was 45 (18-93) years and 45% were male. Of the participants, 22% smoked or had stopped smoking in the six months preceding completion of the questionnaire, while 19% of the participants had hypertension. A total of 68,954 participants did not report CVD or stroke. Of these, 92% (n = 63,393) were at low ten-year CVD risk, and 4.2% (n = 2926) and 3.8% (n = 2635) were at medium and high risk, respectively. A total of 1338 participants reported a previous CVD event, i.e. 744, 586 and 386 reported coronary surgery or suffered from myocardial infarction or stroke, respectively. Of note, some patients reported to have suffered from several forms of CVD and therefore the numbers do not add up directly.
Lipid-lowering drugs and primary prevention
Of the participants without CVD (n = 68,954), 3268 (4.7%) were eligible for LLD. The baseline characteristics of these patients are shown in table 3. Of these, 77% (n=2515) did not report LLD, which was associated with significantly higher median TC (5.9 vs. 4.5 mmol/l; p < 0.001) and median LDL-c (3.9 vs. 2.6 mmol/l; p < 0.001) levels, compared with those reporting LLD use. Those who reported use of LLD had a higher BMI (29 vs. 28 kg/m2 ; p < 0.001) whereas systolic blood pressure was not statistically different (143 vs. 144 mmHg; p = 0.07). These results thus indicate that 2515 of 68,954 (3.6%) participants were not using LLD while the guidelines recommended this. Thus, eight out of ten patients eligible for LLD did not report using LLD.
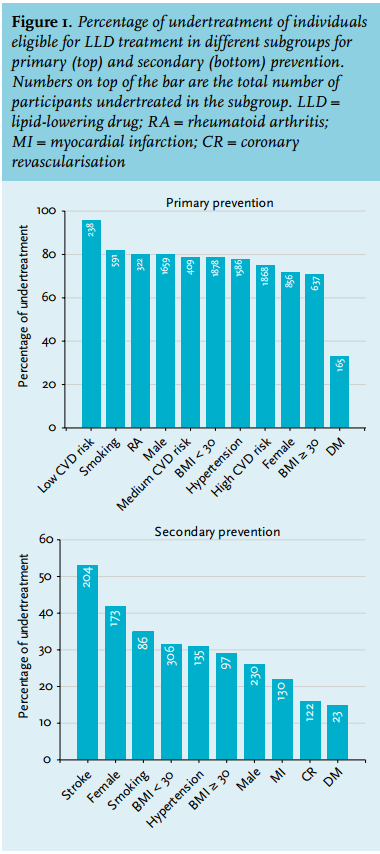
Subgroup analyses showed that 80% of the males and 72% of the females were not treated according to the CVRM guidelines. The percentage of undertreatment of patients with diabetes mellitus was much lower, namely 32% (figure 1).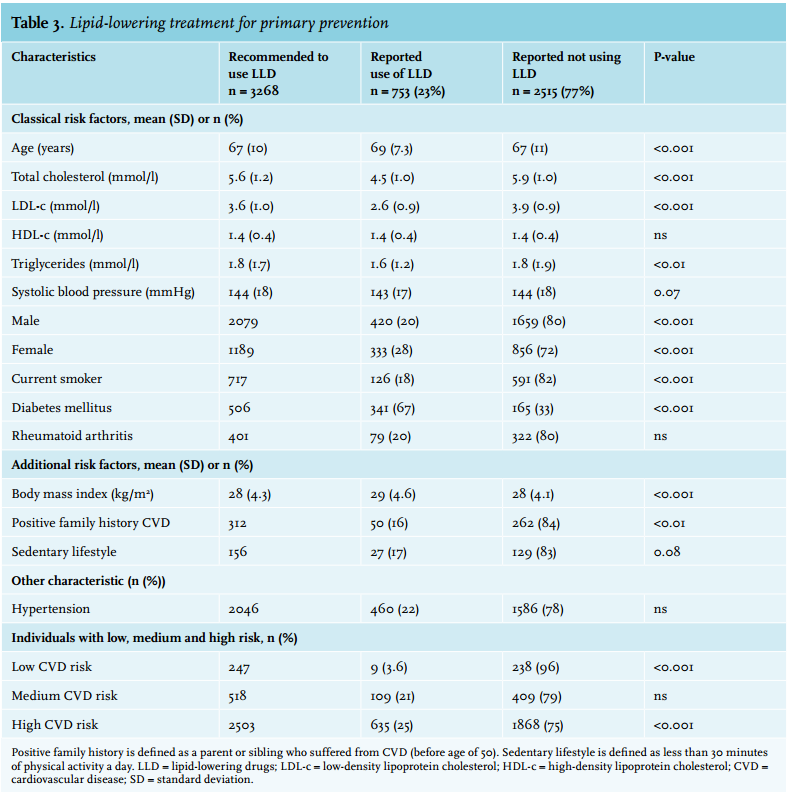
Lipid-lowering drugs and secondary prevention
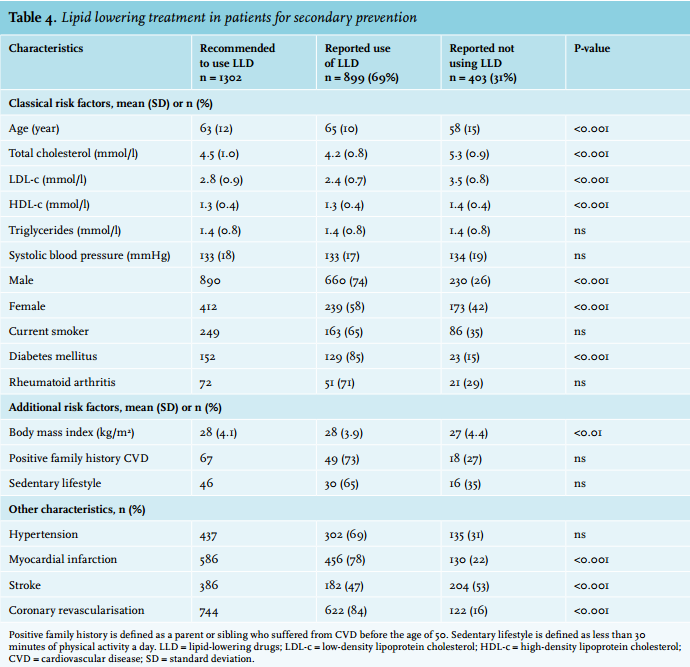
A total of 1338 participants reported to have suffered from CVD or stroke. Of these, 36 patients suffered from stroke but had LDL-c levels ≤ 2.5 mmol/l and therefore had no indication for using LLD. Thus 1302 individuals were eligible for treatment. Of these patients, 403 (31%) did not report use of LLD. Table 4 shows the baseline characteristics of the patients with CVD, who according to the guidelines should receive LLD. The use of LLD in this group was again associated with a significantly lower median TC (5.3 vs. 4.2 mmol/l; p < 0.001) and median LDL-c (3.5 vs. 2.4 mmol/l; p < 0.001) levels, compared with those who did not report LLD, respectively. Thus, out of ten patients eligible for LLD, three did not use LLD. While 26% of the men were not treated according to guidelines, this percentage was significantly higher in females (42%; p < 0.001). Remarkably, 53% of the patients with stroke and LDL-c levels > 2.5 mmol/l did not report the use of LLD. In contrast, diabetes mellitus, coronary revascularisation and myocardial infarction were associated with the most frequent use of LLD (80-85%) (figure 1).
Multivariate logistic regression analysis
The risk factors for undertreatment of LLD, based on multivariate logistic regression analysis, for primary and secondary prevention are shown in table 5. The strongest predictor of not reporting LLD use was a low ten-year CVD risk (OR = 2.4; p = 0.03). These were individuals with TC/ HDL-c ratio > 8. Patients with diabetes mellitus, females, older patients and those with higher BMI were more likely to receive LLD (OR < 1.0; p < 0.05). For secondary prevention, the strongest predictor of undertreatment was being female (OR = 1.63; <0.01). Predictors of LLD treatment following the guidelines are coronary revascularisation, diabetes mellitus, myocardial infarction, higher BMI and higher age (OR < 1.0; p < 0.05).
DISCUSSION
This general population study in the Netherlands showed that, despite clear recommendations, 77% of subjects at high risk of CVD (primary prevention) and 31% with CVD (secondary prevention) did not report receiving LLD. Although these rates of undertreatment have been reported previously, this large and recent study indicates that better action should be taken by healthcare providers and policy makers in the Netherlands.
Primary prevention
According to the CVRM guideline, 4.7% (n = 3268) of the LifeLines subjects without CVD, but with high cardiovascular risk, should have been treated with LLD. Only 23% actually reported using LLD. In a previous study of the general Dutch population, published in 2003, (MORGEN project, n = 61,918; aged 20-59 years), 3.8% were eligible to use LLD.4 Since LDL-c and TC levels increase with age, the higher percentage in our study can be attributed by the inclusion of participants over 59 years of age. In addition, we studied individuals at overall risk of CVD, whereas the MORGEN project focused on hypercholesterolaemia. It is interesting to note, however, that in the MORGEN project, adherence to guidelines was 20% compared with 23% in the current study, which indicates only a slight improvement over the last ten years.
The most obvious reason for the marked undertreatment in our study is the possibility that participants may have never been tested for ten-year CVD risk. Since the most important parameters needed to assess CVD risk (i.e. age, smoking habits, blood pressure, and gender) are easy to obtain, insufficient awareness on the part of the individuals and/or their physicians of CVD risk likely contributed to the observed undertreatment.12
We further assessed whether we could identify subgroups that were prone to undertreatment. Of the patients with diabetes mellitus, 67% reported LLD which is probably related due to the more intense medical care, thus monitoring of plasma lipid levels, in these individuals. In the USA, 52% of individuals with diabetes older than 40 years reported statin use.8 Multivariate logistic regression analysis showed that undertreatment in the LifeLines study was most apparent in younger participants, males, those with lower BMI, and low ten-year CVD risk.
Secondary prevention
Of the patients who suffered from CVD and had a clear indication for LLD, only 69% reported to be actually treated. In EUROASPIRE III,13 very similar data but on a much smaller dataset were reported: 115 out of 167 (69%) Dutch participants reported LLD. Other data collected in the Netherlands in 2007 showed that 53% of the CVD patients were undertreated,14 suggesting a small improvement.
In line with other Dutch studies,5 the current study shows that for secondary prevention 42% of the females did not report LLD, whereas this was only 26% in males. Although CVD is currently the number one cause of death in women in the Netherlands, it appears clear that general practitioners underestimate the risk of CVD in women.15
Our results furthermore show that of the patients who reported stroke, 53% were not reporting LLD use. Remarkably, undertreatment of patients with stroke is even worse in the Oslo Heart study: only 21% of men and 16% of the women were using LLD at age 60, while at age 70 these numbers increased to 44% and 48%, respectively.3 In another Dutch population study it was shown that only 10% of patients with cerebrovascular accident/transient ischaemic accident were undertreated.14 The heterogeneity of these findings may be related to differences in mean age in the respective studies as older people are much more likely to receive a statin. Nevertheless, our observations that both stroke and female gender are associated with undertreatment may need attention in the Netherlands, especially since women generally have a higher overall risk of stroke.16 Multivariable logistic regression analysis showed that physicians prescribing LLD should additionally focus on females and individuals at a younger age.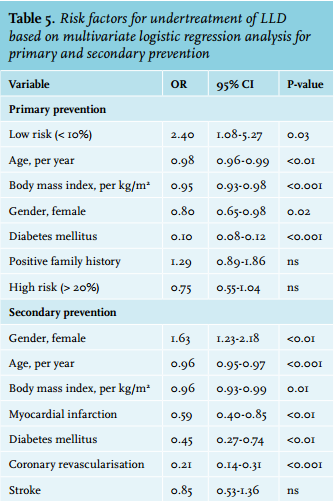
Limitations
The LifeLines questionnaires do not assess peripheral vascular disease, and we could not account for this parameter in our secondary prevention analysis. Next, the information on medication was dependent on the information given by participants. Furthermore, our dataset lacked information on BMI (n = 15), eGFR (n = 262), daily activity (n = 5530) and family history of CVD (n = 23,850). Since these determinants were used in the decision for LLD treatment in the medium ten-year CVD category, this may have resulted in an underestimation of the number of participants with an indication for LLD. We had to decide how to use the guidelines for those patients who had LDL-c levels ≤ 2.5 mmol/l and reported LLD use. We have assumed that these participants had LDL-c levels > 2.5 mmol/l before initiation of LLD treatment, which may have led to overestimating the proportion of proper recommended treatment.
The CVRM guideline used in this study was published in June 2011. However, the inclusion of the LifeLines participants started in 2006 indicating that a significant number of participants entered in a time period in which the previous guideline was applicable. Although the differences between the guidelines are small, the CVRM 2011 guidelines do recommend more aggressive treatment of patients with rheumatoid arthritis. As a result, 145 patients with rheumatoid arthritis were wrongly categorised. This did not affect the overall outcome of our primary prevention analysis (this is only 4.4% of total patients eligible for LLD treatment in primary prevention). In line, table 5 shows that rheumatoid arthritis was not a significant predictor of undertreatment in our multivariate analysis. However, due to the change in the guidelines during the course of our study, the outcome of our study is not applicable for patients with rheumatoid arthritis.
As Lifelines is a population-based study, it should be mentioned that the Dutch CVRM guidelines do not advocate the assessment of a cardiovascular risk profile in all adults. Reasons to assess this are e.g. the presence of hypertension, family history with premature CVD or diabetes. Looking into this specifically, we found however that 90% of participants who were eligible to use LLD, also met criteria for assessing a cardiovascular risk profile (data not shown).
Conclusions and perspective
This large population-based study showed that 77% of the individuals, without CVD, in the Northern three provinces of the Netherlands did not receive LLD while the CVRM guideline would recommend this. This figure is 31% for secondary prevention. While significant progress in the treatment of CVD has previously been reported, our current data showed no signs of further improvement over the last years in the Netherlands.
The results of this study call for improved awareness and better treatment. The development of simple apps to estimate ten-year CVD risk could be of help. However, unfortunately, several key parameters such as plasma levels of HDL-c and LDL-c as well as systolic blood pressure, are currently needed to accurately estimate ten-year CVD risk. Clearly, our data call for large-scale primary prevention programs to improve awareness and treatment of CVD.
DISCLOSURES
This work is supported by Foundation LeDucq (Transatlantic Network, 2009-2014), the Netherlands CardioVascular Research Initiative (CVON2011-2016; Genius) and the European Union (Resolve: FP7-305707; TransCard: FP7-603091-2).
REFERENCES