KEYWORDS
Decision-making, dialysis, elderly, end stage kidney disease, frailty
INTRODUCTION
The process of decision-making concerning dialysis initiation in the elderly is complex and hard to capture in protocols. In elderly patients, bridging to transplantation is usually not an option and prolonging of life must therefore be carefully weighed against the expected quality of life on chronic dialysis. In the last decennium, increasing attention has been drawn to conservative care as an acceptable alternative in selected elderly patients with end-stage renal disease (ESRD).1-3 The Renal Physicians Association and the American Society of Nephrology proposed forgoing dialysis in patients with a very poor prognosis, including those with high comorbidity, severely impaired functional status and severe malnutrition.4 However, in elderly patients without these contraindications, the decision-making process of commencing dialysis remains challenging. Elderly patients treated with conservative therapy may spend less time in hospital compared with elderly patients receiving dialysis therapy and they are more likely to die at home or in a hospice instead of in a hospital compared with dialysis patients.5 Although age has been included in prognostic models in dialysis patients,2 other studies found that age per se was not associated with early mortality or withdrawal in the elderly.6 Elderly patients may exhibit more comorbidities, and the prevalence of functional and cognitive impairments in this group is high.5,7,8 Frailty,9 cognitive impairment,10 comorbidities11 and impaired mobility12 have been shown to be of prognostic value for early mortality and hospitalisation in the dialysis population. Despite the growing proportion of older dialysis patients, few studies have focused specifically on their prognostic relevance in the elderly population.
In oncology, assessment of geriatric impairments, such as cognition, mobility, (instrumental) activities of daily living (ADL), mood, nutrition, comorbidities and social environment, before the start of therapy can aid in identifying patients at risk for chemotherapyrelated toxicity13 and postoperative complications in surgical oncology.14 A systematic review showed that in six studies focusing on the effect of geriatric evaluation in decision-making in oncology, such a geriatric evaluation changed the initial treatment decisions in a median of 39% of patients. In approximately two-thirds of patients this resulted in a more conservative treatment plan.15 A questionnaire among oncologists and oncology nursing specialists in the Netherlands revealed that geriatric evaluation was used in two-thirds of participants, although often not systematically due to a lack of time, or limited availability of geriatricians.16
Little is known about nephrologists’ considerations in the decision-making process of dialysis initiation in the elderly. Previous surveys among nephrologists revealed that patient preference, the presence of severe conditions, vascular dementia and a poor physical functioning were important determinants in deciding to withhold dialysis.17,18 To what extent other frequently encountered geriatric problems such as mood disturbances, ADL impairment, frailty and (mild) cognitive impairment influence the decision-making of nephrologists is not known. For this reason, a survey was conducted to assess whether these issues are evaluated systematically before dialysis initiation and whether nephrologists would consider further evaluation in the elderly supportive in the decision-making process.
SUBJECTS AND METHODS
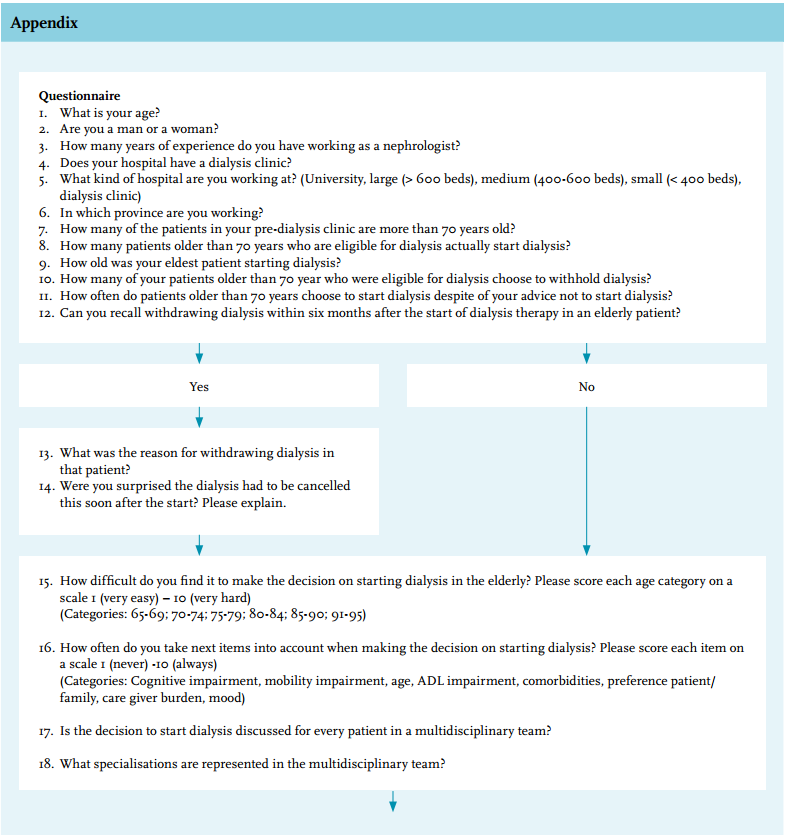
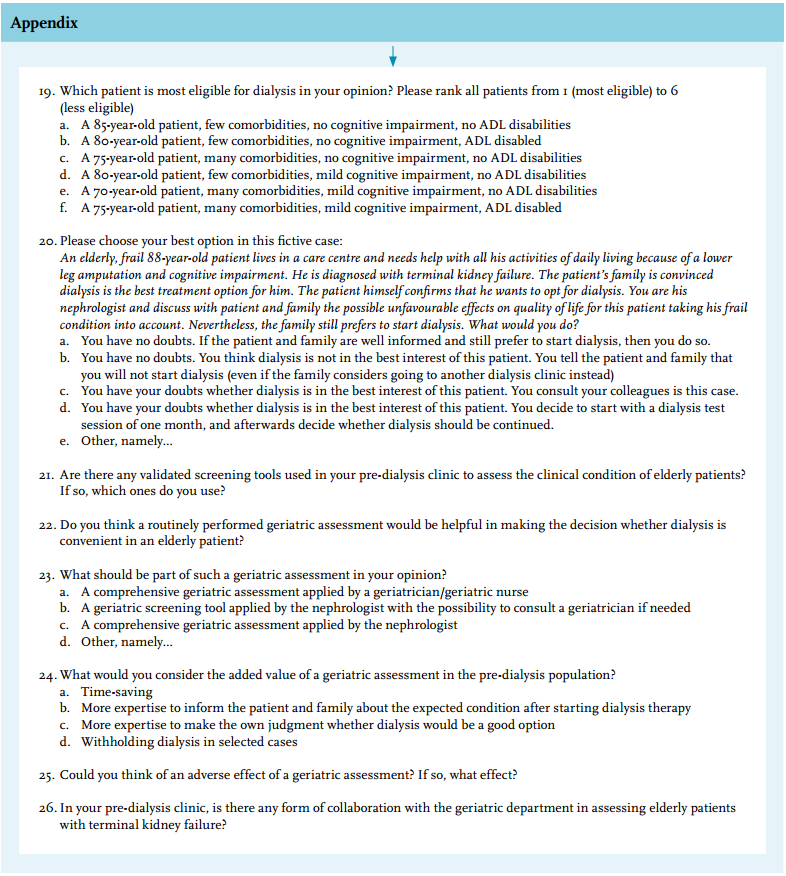
An internet-based anonymous questionnaire for nephrologists was developed, focusing on the main issues related to initiation of dialysis in elderly patients derived from clinical practice and the literature.17-20 The survey consisted of 25 questions (Appendix) about decision-making itself and the potential role of a geriatric assessment in this process. Data were collected on characteristics of the responding nephrologists, including years of experience and facility type, and demographics of the dialysis population. The survey took about 15 minutes to complete. In February 2014, all members of the Netherlands Federation of Nephrology (NfN), 298 nephrologists in total, were requested by email to respond to the questionnaire. With only a few exceptions, all registered nephrologists in the Netherlands are members of the NfN. No fee was paid to respondents. All responses were entered into SPSS statistical package version 22 (IBM SPSS Data Collection, Chicago, Illinois, USA). To compare for differences between groups, a Student’s t-test was used for continuous variables; for nominal variables, the chi-square test was used. For not normally distributed variables a Mann-Whitney U test was used. All other results are presented as descriptive data.
RESULTS
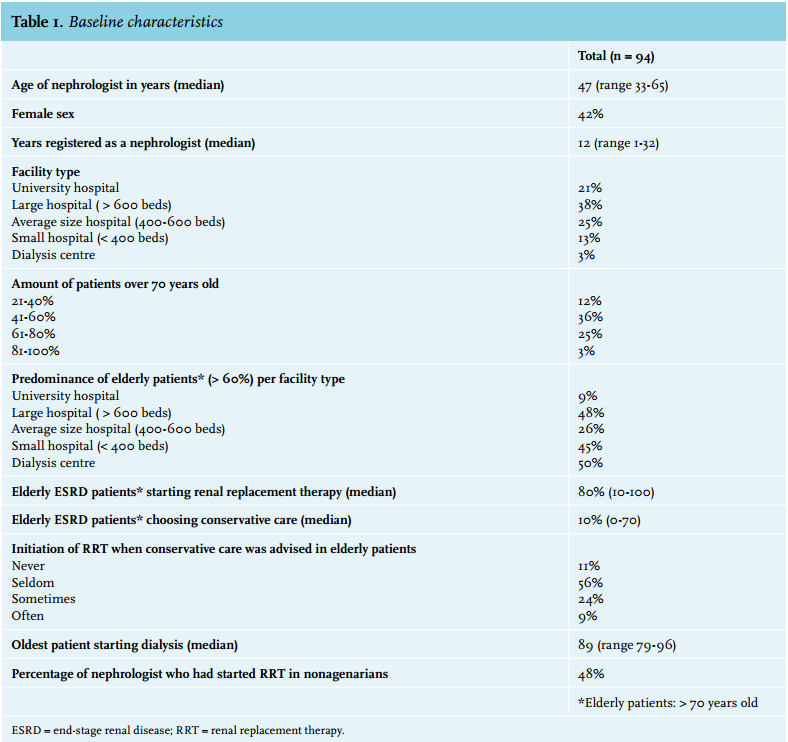
CharacteristicsA total of 94 nephrologists from the Netherlands filled out the questionnaire (response rate 32%). All types of dialysis care facilities (university hospital, (non) teaching hospital, commercial dialysis centre), from all regions of the country were represented. The mean age of the participants was 47 years (33-65 years). The characteristics of respondents and their dialysis population are presented in table 1. One-third of the respondents estimated that the majority of their prevalent dialysis patients are over 70 years of age. Of all ESRD patients over 70 years, respondents estimated that a median of 80% (range 10-100%) would eventually start renal replacement therapy; 40% of respondents had started dialysis in one or more nonagenarians. Mean age of the dialysis population did not differ significantly between facility type and region.
Decision-making concerning dialysis in the elderly
Opinions about the level of difficulty of decision-making concerning dialysis in the elderly differed widely (median score 4 (range 1-10) on a scale from 1-10). The process of decision-making almost always included consultation of a multidisciplinary team, consisting of a nephrologist, a specialised nurse, a social worker and a dietician (95%). In some clinics a psychologist, a spiritual worker or a pharmacist complemented the team. In 8% a geriatrician was involved on a regular or a consultative basis. When dialysis was considered unfavourable because of a poor prognosis, only 11% of nephrologists estimated that older patients would always accept the recommendations of the nephrology team for conservative care instead of renal replacement therapy, while 9% experienced elderly patients often insisted on starting dialysis despite a contrary recommendation.
Different strategies were chosen in a hypothetical case of a frail older patient, in whom dialysis initiation was considered unfavourable, but no agreement could be reached about conservative therapy. Six percent of the nephrologists would initiate dialysis, since the patient and family made a well-informed choice for this option. Ten percent would refuse to start dialysis, regardless of the patient’s wishes, since dialysis might be harmful in this frail patient. Most respondents remained unconvinced of either option. They would consult colleagues (42%) or initiate a dialysis test session for 1-3 months (37%) before making a decision in this particular case. Five percent of nephrologists would consult a geriatrician.
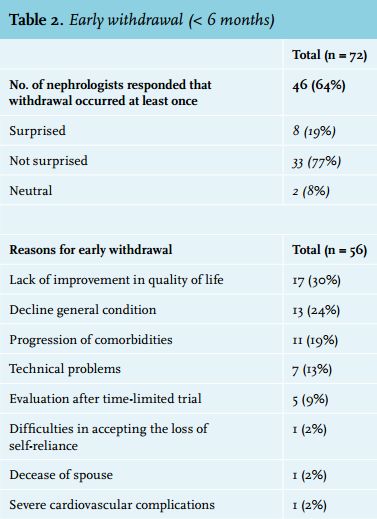
Of all respondents, 64% estimated that within their own dialysis population early withdrawal (within 6 months) had occurred at least once in an elderly patient (table 2). The main reasons for withdrawal were lack of improvement in quality of life (30%) or decline of the general condition (24%). Less often mentioned were progression of comorbidities or newly diagnosed comorbidities (19%) or technical problems involving dialysis treatment (13%). In 9% of cases withdrawal occurred after a time-limited trial. Other reasons for early withdrawal are listed in table 2. In 77% of the cases of early withdrawal, this was not unexpected to the nephrologist involved. The most frequently mentioned reason for starting dialysis despite hesitations was the inability to reach consensus with the patient and/or relatives to choose maximum conservative management.
Factors included in dialysis decisions in elderly patients
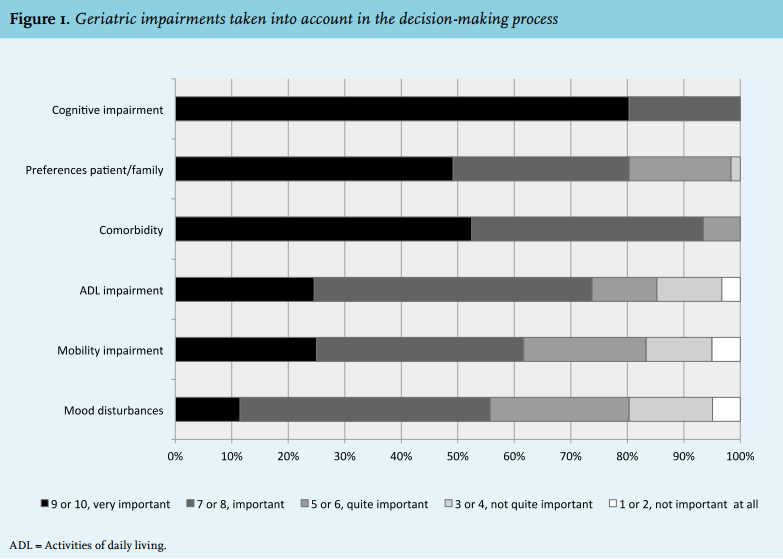
Geriatric impairment was considered a (very) relevant issue and was always taken into account by nephrologists when deciding whether a patient would be eligible for dialysis (figure 1). On a scale from 1 (not important at all) to 10 (very important), cognitive impairment scored a median of 10 (range 6-10). Preference of the patient and family (median 10 (range 3-10)) and comorbidities (median 9, (range 5-10)) were also considered (very) relevant in decision-making by almost all respondents. Most nephrologists answered that they take into account impairments in activities of daily living (ADL) (median score 8, (range 2-10)), mood disturbances (median 7, (range 2-10)) and mobility impairment (median 7, (range 1-10)). The patients’ age was also considered relevant in decision-making, with a median score of 7 (range 1-10).
As reflected by the wide range, the opinions regarding these geriatric impairments and age were divided. Caregiver burden (median 6, (range 1-10)) was considered least relevant. In a fictive case of a frail elderly patient considering dialysis, age was considered less relevant than cognitive impairment, comorbidity and ADL impairment. Decision-making seemed to be most difficult for patients aged 76-90 years (median 4 (range 1-10)), and easier for younger and older patients (median 3 (range 1-10)). Yet, the differences per age category are small and the ranges are wide (figure 2). The wide range is most distinct in the youngest and the oldest age category, due to the fact that some physicians consider decision-making more difficult with ascending age (40%), whereas others (30%) considered it less difficult when patients get older. We could not explain those different patterns by age of the nephrologist, years of experience and type of dialysis facility.
Additional evaluation of geriatric impairments
More than half of the respondents (56%) considered evaluation of geriatric impairments to be of potential benefit in the decision-making process before starting dialysis in elderly patients. Nephrologists in favour of a geriatric evaluation were generally younger (mean age 45.0 vs. 49.9 years, p = 0.02). This opinion was not influenced by gender. Arguments in favour of and against a geriatric evaluation are shown in table 3. Systematic evaluation of geriatric problems was expected to improve estimations about the condition after starting dialysis, which could help in informing the patient and his or her relatives (62%), in making one’s own estimation of treatment success (47%) and in more often withholding dialysis in selected cases (11%). On the other hand, respondents found that different opinions between physicians could work counterproductively (33%) and it could be time consuming (19%). Of the nephrologists, 19% felt a geriatrician would lack sufficient knowledge regarding dialysis.
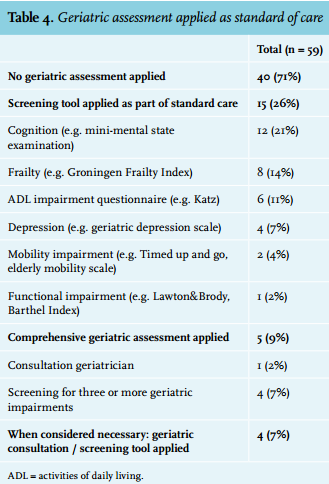
When asked about the ideal form of this evaluation, 78% of respondents preferred application of a short screening tool in the pre-dialysis clinic, supplemented with consultation of a geriatrician when needed while 23% preferred a comprehensive geriatric assessment, either performed by a geriatrician (18%) or a nephrologist (5%). Such an assessment was already performed as standard of care by 9% of respondents, while 26% of the respondents reported using one or more tools to assess one or more geriatric domains, most frequently focusing on cognitive impairments (e.g. the Mini Mental State Examination, MMSE) or frailty (table 4). Other geriatric impairments being tested were: impairments of ADL, depression, functional impairment, and mobility impairment.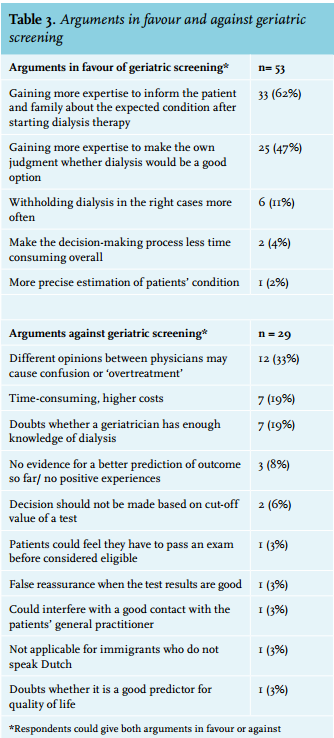
DISCUSSION
This national survey revealed that geriatric impairments are considered important items influencing the decision-making process of dialysis initiation in the elderly, outweighing age as relevant item needing consideration. The majority of nephrologists (56%), especially younger colleagues, consider screening for impairments in the elderly population useful, but few use a geriatric assessment or screening instrument in the work-up of elderly pre-dialysis patients.
In general, decision-making in elderly ESRD patients was not considered difficult (median 4 (range 1-10)) but 89% of respondents at least occasionally reported difficulties in reaching consensus regarding treatment decisions. The ‘Clinical Practice Guideline on Shared Decision-Making in the Appropriate Initiation of and Withdrawal from Dialysis’ proposes to consider a time-limited trial when no consensus can be reached or the patient prognosis is uncertain.19 However, the achieved quality of life after starting dialysis may not turn out as expected.21 In a Canadian study of 584 ESRD patients (age 68 ± 14 years, mean time on dialysis 27 ± 22 months), 61% reported regretting their decision to start dialysis.22 When looking at all cases of early withdrawal based on our survey, 77% were not unexpected to the responding nephrologist. This implies starting dialysis despite some hesitations about the benefits of dialysis is not exceptional. Worldwide, based on the Dialysis Outcomes and Practice Patterns Study (DOPPS), most cases of withdrawal occur early after initiation of dialysis and account for 3-39% of deaths within the first 120 days, with a wide range between countries.23 A time-limited trial may facilitate the decision-making process by postponing the definitive decision, but it will not prevent early withdrawal. These findings underline the need for a careful consideration of what to expect before the start of dialysis or a time-limited trial.
In our survey, cognitive dysfunction was considered most relevant of all geriatric impairments in treatment decision. Dementia is a known predictive factor for poor survival in patients initiating dialysis, with a two-year survival of 24% vs. 66% in patients without dementia (p < 0.001).10 Cognitive impairment may compromise therapy adherence, diet and fluid restrictions, may lead to behavioural disturbances and higher care burden. Unexpected rapid decline of cognitive function was reported as a reason for early withdrawal, although this was not mentioned often (5%). Screening for cognitive function prior to dialysis initiation may help in obtaining an estimation of the patient’s prognosis, the expected benefits of dialysis therapy and the risks of unwanted treatment outcomes.8 A previous study found that cognitive impairment is largely underdiagnosed in dialysis and ESRD patients.8 In our survey, only 21% of respondents reported using an objective instrument to assess cognitive function before dialysis initiation, although almost all considered it (highly) relevant to treatment decisions. A simple, validated test for cognition in the ESRD population is currently lacking. The Montreal Cognitive Assessment (MoCA), a brief cognition screening test, recently showed good sensitivity and specificity for cognitive impairments in prevalent dialysis patients and performed better than the better-known MMSE.24 Whether this test will be of added value in decision-making for the elderly ESRD population is yet to be determined.
In addition to the disabilities previously mentioned to be relevant in the decision-making process,17,18 such as comorbidity, vascular dementia and a poor physical functioning, this survey shows mood disturbances and ADL impairment are also found to be relevant items needing consideration before starting dialysis therapy in the elderly. Depression is highly prevalent among dialysis patients, and undertreatment and underdiagnosis are common.8 Both depression25 and ADL impairment26 are associated with adverse outcome in dialysis patients and early awareness might therefore be relevant in evaluating the patient prognosis, implementing early interventions and improving quality of life. As with cognition, it is not common practice to objectively assess these disabilities using a screening instrument. There were some initiatives (14%) to assess frailty, the phenotype of general decline in the ageing population.27 Over the last decade, frailty has been recognised as a predictor for poor outcome in the dialysis population.9 Although as yet no screening instrument has been validated for measuring frailty in the ESDR population, these initiatives may reflect the desire for a simple screening method for the overall condition in the elderly.
The present study has several limitations. The response rate of this nationwide survey was only 32%. This is a well-known issue in survey research. For example, previous international nephrology surveys yielded 50 or fewer responses in the Netherlands and other participating countries.17,20 Responders and non-responders may differ in their interest in geriatric nephrology. This may have led to overestimation of the importance nephrologists seem to assign to geriatric impairments and the potential added value of screening for these impairments. A survey can provide only a simplified view of the complexity of daily practice. In an attempt to simulate real world decisions, this survey presented the questions concerning the importance of geriatric impairments in two different ways. For example, question 16, focusing on the value of the independent geriatric impairments, and question 19, incorporating geriatric impairments in a context of more complex decision-making, both showed geriatric impairments were considered more relevant than age itself in decision-making in elderly ESRD patients.
CONCLUSION AND POTENTIAL IMPLICATIONS
In this survey among Dutch nephrologists, geriatric impairments were shown to be considered relevant to the decision-making process regarding dialysis initiation in the elderly. Nephrologists are open for the use of screening instruments for geriatric problems, but structural, objective assessment of the presence and severity of geriatric impairments is not customary. This may be due to lack of validated screening tools in the ESRD and dialysis population. As geriatric impairments are associated with adverse outcome in dialysis, future research should focus on validating existing screening instruments in this patient population or developing new tools that take factors specifically relevant to renal disease and dialysis into consideration. In addition, it remains to be investigated whether the incorporation of some form of geriatric assessment in the decision-making process regarding initiation of dialysis will be useful in identifying vulnerable patients better suited for best supportive care.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES