CASE REPORT
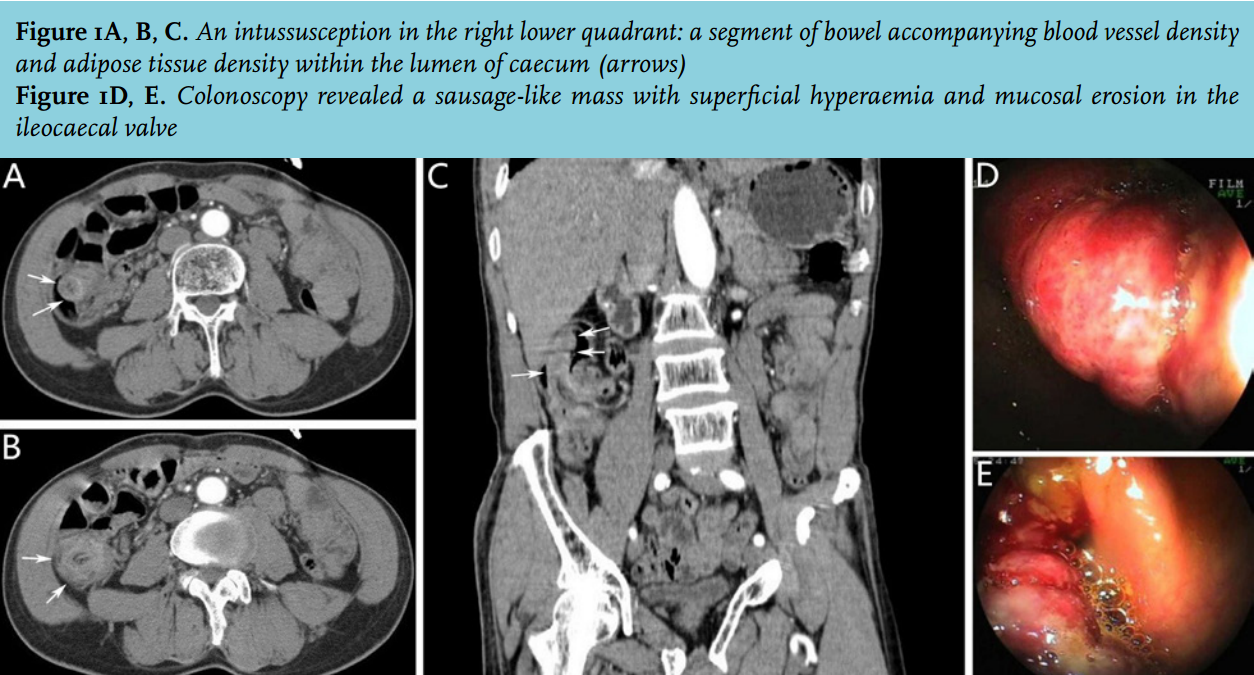
A 64-year-old man presented with a four-day history of intermittent abdominal pain and melaena. The patient had no past history of cancer and no family history of colorectal cancer. Physical examination revealed mild periumbilical and right lower quadrant abdominal tenderness without rebound tenderness. Laboratory examination showed no abnormality. Contrast-enhanced computed tomography (CT) (figure 1A, 1B and 1C) showed an intussusception in the right lower quadrant: a segment of bowel accompanying blood vessel density and adipose tissue density within the lumen of caecum (arrows). Colonoscopy (figure 1D and 1E) revealed a sausage-like mass with superficial hyperaemia and mucosal erosion in the ileocaecal valve.
DIAGNOSIS
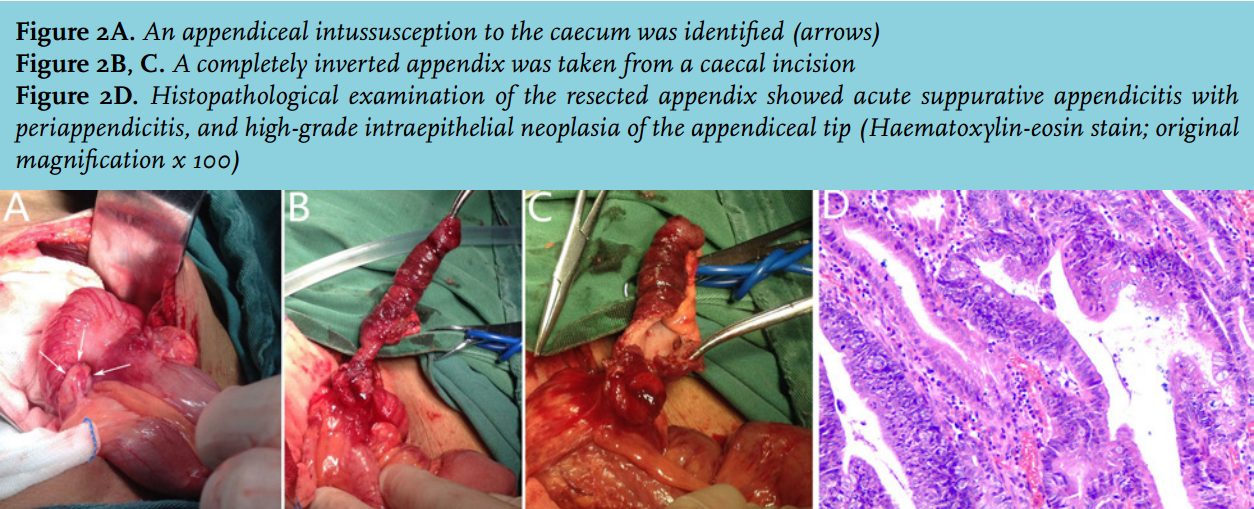
The patient underwent exploratory laparotomy following the initial diagnosis, at which time an appendiceal intussusception to the caecum was identified (figure 2A) (arrows). The intussusception could not be manually reduced, and so a completely inverted appendix was taken from a caecal incision (figure 2B and 2C) and an appendectomy was performed. Histopathological examination of the resected appendix showed acute suppurative appendicitis with periappendicitis, and high-grade intraepithelial neoplasia of the appendiceal tip (figure 2D), suggesting it as the cause of the intussusception. The postoperative course was uneventful. Appendiceal intussusception is a very rare entity, with an incidence of 0.01% in 71,000 human appendix specimens.1 It occurred less often in adults than in children, and the diagnosis is rarely made preoperatively.2 It has also been reported that appendiceal intussusception in adult women is mainly due to endometriosis, and in children is mainly due to inflammation.3 Appendiceal intussusception may mimic an ileocolic intussusception. Contrast-enhanced CT and colonoscopy may help to precisely identify the causative lesion preoperatively.4 A firm diagnosis of an appendiceal intussusception to the caecum induced by high-grade intraepithelial neoplasia could be established fundamentally. It was based on the intraoperative exploration and the histopathological examination.
In adults, intussusception is usually associated with a neoplastic lead point and requires surgical exploration with resection.1,5 Our case was considered intraoperatively to be caused by a pure inflammatory lesion and not a neoplastic entity. Thus a simple appendicectomy with a caecal incision was performed. As a result of the postoperative histopathological examination, which revealed acute suppurative appendicitis with periappendicitis, and high-grade intraepithelial neoplasia of the appendiceal tip, a second unnecessary radical resection was avoided. Open surgery should be recommended for this type of appendiceal intussusception, which is described as a completely inverted appendix into the caecum and cannot be manually reduced. Otherwise, when dealing with this type of appendiceal intussusception, a laparoscopic procedure should be completed by the experienced laparoscopic surgeons.
REFERENCES