KEYWORDS
25-hydroxyvitamin D levels, vitamin D deficiency, low-energy fracture, osteoporosis
INTRODUCTION
Vitamin D deficiency is common in elderly patients with a fracture caused by a low-energy trauma. Bours et al. found a vitamin D deficiency (< 50 nmol/l) in 64% of their patients, all with a recent fracture.1 Severe vitamin D deficiency is associated with muscle weakness, bone pain, and an increased risk of falls and fractures.2 In general, the supply of vitamin D mainly relies on exposure to the sun, body mass index (BMI) and skin colour.3
The recent Dutch guidelines on osteoporosis and fracture prevention advise a daily intake of 800 IU cholecalciferol for people over 50 years of age and those suffering from osteoporosis. They additionally recommend a 25-hydroxyvitamin D level target value of at least 50 nmol/l.4 However, several authors consider the optimum level to be > 75 nmol/l, since it is considered to be the minimum level to prevent falls.5 All in all, considering its impact on preventing falls and fractures, vitamin D supplementation is of great importance.
No consensus has been reached on whether a post-treatment control level should be established when a mild or severe vitamin D deficiency has been diagnosed, or on what the optimum daily dose of vitamin D supplementation should be in clinical practice.2 Van den Bergh et al. recently proposed to establish a control 25-hydroxyvitamin D level after three months of supplementation and, if necessary, to adjust the recommended dose of cholecalciferol.6 They based their proposal on the finding that, in a low-energy fracture patient population, the optimal level of > 50 nmol/l was often not reached with a daily dose of 800 IU.1
A meta-analysis showed that with a 25-hydroxyvitamin D basal level of < 50 nmol/l, vitamin D supplementation with 400 IU/day led to an average increase in vitamin D levels of 12 nmol/l.5 So far, there have been few reports on the effect of a relatively low dose (400-800 IU a day) of oral vitamin D supplementation on the increase of 25-hydroxyvitamin D levels in patients > 50 years with a (low-energy) fracture. The objective of this study was to examine the following research questions: A: What is the increase of the 25-hydroxyvitamin D level after supplementation with a daily dose of 800 IU of cholecalciferol in patients with a severe vitamin D deficiency (< 30 nmol/l) and a low-energy fracture? B: What percentage of patients will reach the minimum target value of 50 nmol/l? C: Which factors affect the increase of the 25-hydroxyvitamin D level? Factors that were expected to influence this increase were body weight, BMI, renal function, gender, age, season and 25-hydroxyvitamin D basal level.
METHODS/PATIENTS
Since 2007, the St. Antonius Hospital screen all patients over 50 years of age with a low-energy fracture (except in fingers, toes and metatarsal bones) at the fracture-osteoporosis outpatient clinic for the presence of osteoporosis/osteopenia, by means of DEXA and X-rays of the lumbar and thoracic vertebrae. All patients are asked to complete a questionnaire on known risk factors for osteoporosis/osteopenia. In addition, relevant laboratory tests are run, including a measurement of the 25-hydroxyvitamin D level. Serum 25-hydroxyvitamin D levels were determined on a high-performance liquid chromatography (HPLC) column with two mobile phases (Chromosystems, Munich, Germany) after a purification step. Data on serum 25-hydroxyvitamin D levels were collected retrospectively. The patients with a serum 25-hydroxyvitamin D level < 30 nmol/l were referred to the rheumatologist to further investigate the cause of their severe vitamin D deficiency. For the purposes of this study, patients were not allowed to take supplements containing any vitamin D < 3 months prior to their first vitamin D measurement. All patients were prescribed a supplement of 800 vitamin D IU/day (12 received 880 IU/day).
For all patients included in this study, a second measurement of the 25-hydroxyvitamin D level was done during their visit to the rheumatologist. Exclusion criteria for this study were: a known malabsorption syndrome, primary hyperparathyroidism, hyperthyroidism, an eGFR < 40 ml/min, any reasonable doubt on the intake of vitamin D and lack of a second vitamin D measurement after treatment.
DATA ANALYSIS
Standard descriptive statistical methods were used. To determine the association between two continuous variables, a linear regression was calculated with the correlation coefficient (r) and p-value for the beta of the independent variable.
A student’s T-test was used to calculate the association between a continuous variable and a binomial variable, and for a multiple category variable, the ANOVA test for an ‘overall’ p-value was used; to further explore the associations we computed Tukey multiple comparisons paired p-values and a p-value for linear trend.
RESULTS
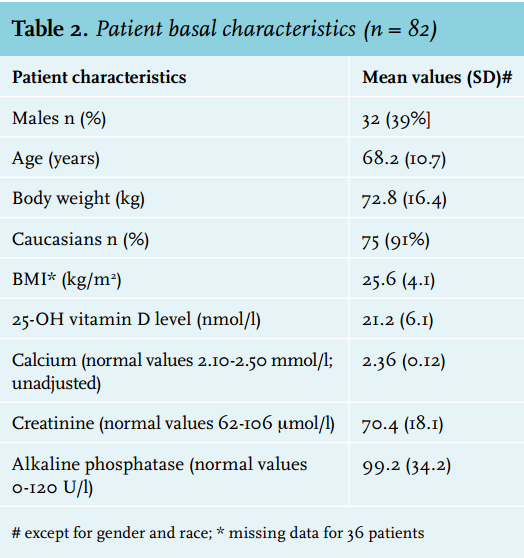
Between January 2008 and June 2011, 134 patients who met the inclusion criteria for this study and had a 25-hydroxyvitamin D level < 30 nmol/l were seen at the fracture-osteoporosis outpatient clinic. Ninety of these patients had both an evaluation by the rheumatologist and a second 25-hydroxyvitamin D measurement. After exclusion of eight patients (see table 1 for the reasons), 82 patients were included in the final evaluation. An overview of the basal characteristics of the patients is provided in table 2. The baseline 25-hydroxyvitamin D level had an inverse correlation (r = - 0.241, p = 0.0291) with body weight but, due to missing data on height, not with BMI. From the 82 patients included, a second 25-hydroxyvitamin D measurement was performed after a mean period of 9.8 (SD 5.3) weeks. All patients showed a highly variable increase in 25-hydroxyvitamin D level, with an average increase of 48 nmol/l (SD 21; range 8-101).

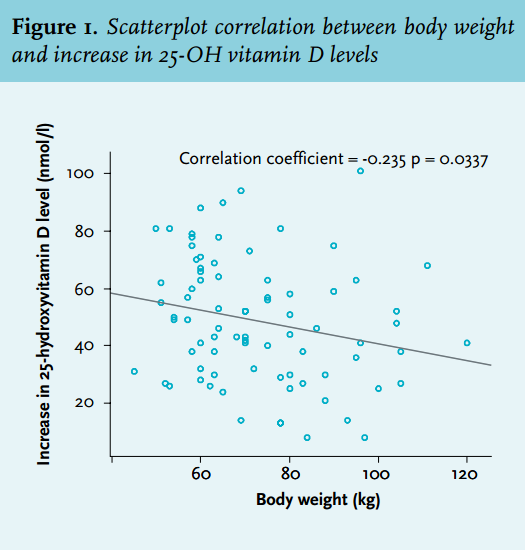
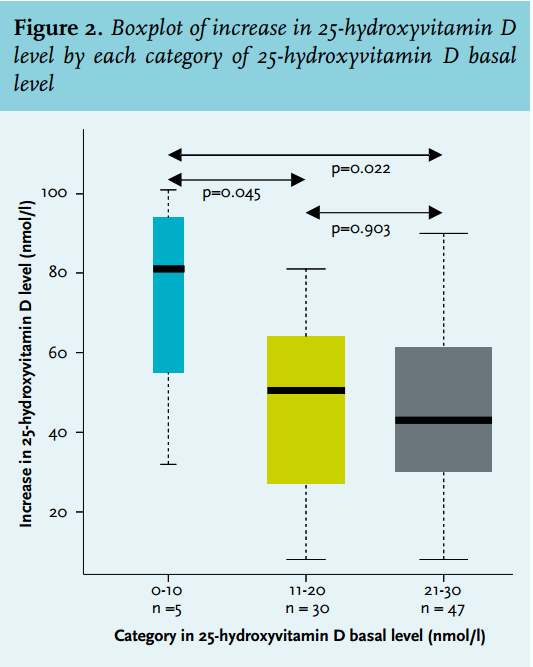
Only 37 patients (45.1%) reached a 25-hydroxyvitamin D level of > 50 nmol/l. There was an inverse correlation between the increase in vitamin D levels and body weight (r = -0.225, p = 0.0417). We also found an inverse correlation between the individual 25-hydroxyvitamin D basal level and the increase in 25-hydroxyvitamin D levels (r = -0.235, p = 0.0337; figure 1). When comparing different subgroups by their basal vitamin D level, the group that had the lowest basal values (0-10 nmol/l, mean increase 73 [SD 28]) clearly showed a stronger increase than both the middle (11-20 nmol/l, mean increase 48 [SD 22]) and the highest (21-30 nmol/l, mean increase 46 [SD 19]) groups [p for trend = 0.0298, figure 2]). The degree to which the level increased was not related to gender, BMI (missing data), age, season (April to October versus November to March) or renal function (data not shown).
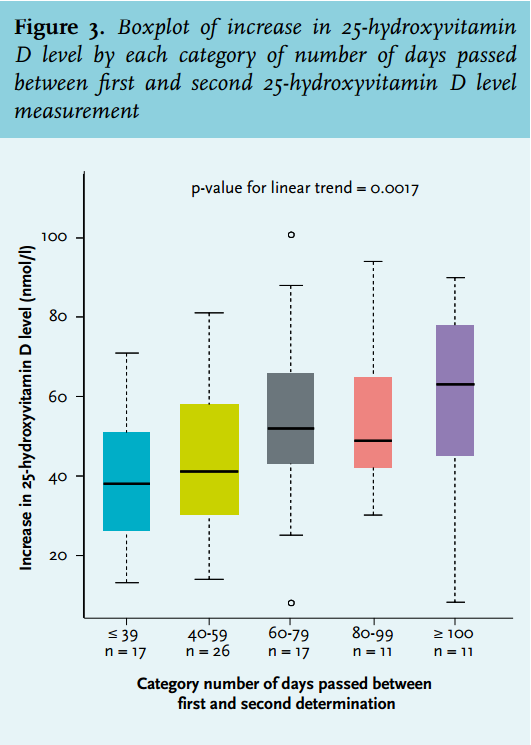
Statistical analysis showed a significant positive correlation between the increase in 25-hydroxyvitamin D level and the number of days that passed between the first and second measurement (r = 0.246, p = 0.0260). Even after three months of vitamin D supplementation, a plateau phase was still not reached (figure 3).
DISCUSSION
In our mostly Caucasian and female population with a mean age of 68.2 years and severe vitamin D deficiency (average value 21.2 nmol/l), after supplementation with 800 IU/day of vitamin D, we observed a mean increase of 48.5 nmol/l after an average of 9.8 weeks. These results are in concordance with those found by Chel et al., 7 who reported a mean increase of 34.9 nmol/l after two months and 44.9 nmol/l after four months after supplementation with 600 IU/day of vitamin D in nursing home patients (mean age 84 years). In patients with various rheumatic diseases and a mean age of 68 years, vitamin D levels increased from 30.8 to about 60 nmol/l after at least six months of treatment with vitamin D 800-1000 IU a day.8
After supplementation with 800 IU/day, Lips et al. observed a larger increase in the 25-hydroxyvitamin D level (namely from 23.7 nmol/l to 80 nmol/l) after three months in elderly patients (> 80 years) living in nursing homes or old peoples’ homes, who likely had a better compliance.9 Gallagher et al. recently reported in a placebo-controlled study with healthy post-menopausal women (mean basal vitamin D level 38.2 nmol/l) that after three months of supplementation with 800 IU vitamin D a day, a vitamin D level of > 50 nmol/l was reached in 97.5% of the cases.10 These results obviously cannot be translated to clinical practice in fracture patients who are for the most part older and have lower basal vitamin D levels. In daily practice, it is a clinically relevant question to ask whether the generally recommended dosage of 800 IU vitamin D per day11 is sufficient for elderly patients with a recent fracture and a severe vitamin D deficiency.
We are not aware of any other reports on the increase of vitamin D levels after supplementation in elderly fracture patients with very low basal vitamin D levels. In our study, the patients with the lowest 25-hydroxyvitamin D basal levels showed the highest increase after supplementation. This is in concordance with results previously reported in the literature on this subject.2 In the present study, no plateau phase was reached after three months of supplementation. Vieth et al. showed that healthy volunteers (mean age 41 years) taking 1000 IU/day of vitamin D reached a plateau phase of vitamin D after three months, with vitamin D levels increasing from 40.7 to 68.7 nmol/l.12 However, in a study with elderly subjects, Lips et al. reported on a plateau phase after 6-9 months of supplementation.9 A control measurement of vitamin D should therefore be conducted after at least three months of supplementation3 or, in our opinion, perhaps preferably after six months.
Fewer than half (45.1%) of our patients reached the generally advised 25-hydroxyvitamin D target value of 50 nmol/l (after ten weeks). We do realise that this threshold of 50 nmol/l is arbitrary and that some advocate higher target levels such as 75 nmol/l.6 As expected, a level of > 75 nmol/l was reached in only a minority of our patients (12.2%). We do agree that the follow-up time was probably too short to reach a new plateau level of vitamin D.
Despite that, it seems likely that the generally used and recommended dosage of vitamin D of 800 IU/day is too low and that treatment should perhaps consist of a higher, possibly loading, dose,6,8 especially in cases of severe deficiency and obesity.5 Van Groningen et al. found an increase of vitamin D from 20.5 to 74.8 nmol/l after eight weeks following a loading dose of vitamin D (total dosage 100,00-200,000 IU) in vitamin D-deficient adults. The target levels of vitamin D of 50 and 75 nmol/l were reached in 76% and 48%, respectively.13 These figures are obviously higher than in our study. Of course, it may also be considered to adjust the dosage of vitamin D suppletion according to the basal vitamin D levels.
We identified an inverse correlation between body weight and basal vitamin D levels. Indeed, it is already known that obese subjects have lower basal vitamin D levels because they have a larger distribution volume.13,14 It has been demonstrated in recent literature that also the increase in the 25-hydroxyvitamin D level negatively correlates with body weight and/or BMI.11,15 Indeed, in our only slightly obese patients (BMI 25.4), we found a negative correlation between body weight and the increase in vitamin D levels. We did not find such a correlation between this increase and BMI due to a large quantity of missing data on height. The most important limitations of our study are its retrospective format and the follow-up time < 100 days, which is too short to reach a new plateau level of vitamin D. In addition, there was no information on dietary intake of vitamin D and compliance of intake of vitamin D medication. The study’s strengths are: it reports on a clinically relevant question in daily practice and that it was investigator driven without any financial support.
CONCLUSIONS
In conclusion, we have shown that after a dose of 800 IU/day of vitamin D, only 45.1% of the elderly fracture patients with a severe vitamin D deficiency reached the advised 25-hydroxyvitamin D level of > 50 nmol/l after an average of ten weeks. The increase in vitamin D level had an inverse correlation with basal vitamin D levels and body weight, and was expectedly associated with the duration of supplementation. Based on our data and data from the literature, we propose taking a second measurement of the vitamin D level after at least six months of supplementation, with dosage adjustment.
DISCLOSURES
The authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES