INTRODUCTION
Peliosis hepatis is a rare vascular condition of the liver characterised by the presence of cystic blood-filled cavities distributed randomly throughout the liver parenchyma. The term originates from the Greek ‘pelios’ which means ‘lead-coloured’ (extravasated blood). Peliosis is most commonly found in the liver, but can also involve other organs. An aetiology remains unclear in up to 50% of the patients. Peliosis hepatis has been described primarily in patients on androgenic steroid medication and patients with tuberculosis.1,2 Nowadays, it has been associated with multiple drugs (such as oral contraceptives as in our patient), chemicals, bacterial and HIV infections, haematological disorders, malignancies and renal transplantation.3,4 Some studies have described the prevalence of peliosis hepatis in patients with associated conditions, such as 0.2% in patients with tuberculosis1,2 and 0-22% after renal transplantation.4 No numbers are known on the prevalence of peliosis hepatis in association with oral contraceptives. In the described patient, the diagnosis of peliosis hepatis was not made by the imaging modalities, which suggested metastases, but by liver biopsy. Peliosis hepatis should nowadays be considered in the differential diagnosis of suspected hypervascular liver lesions diagnosed by imaging, in women with a history of long-term use of oral contraceptives.
|
What was known on this topic? What does this case add? |
|
|
CASE REPORT
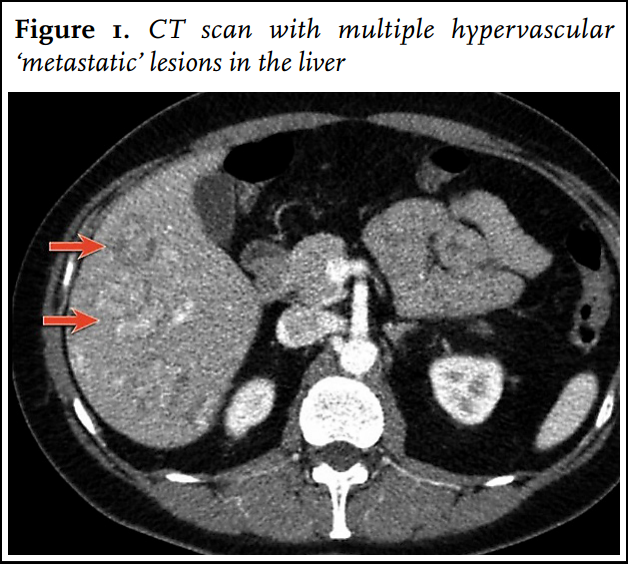
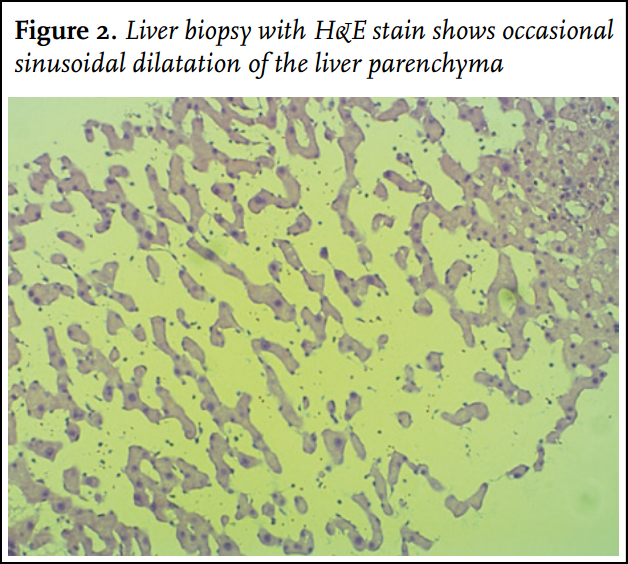
An otherwise healthy 47-year-old woman presented for evaluation of an elevated erythrocyte sedimentation rate and abnormal liver function tests in the outpatient department. She reported vague epigastric pains and nausea. She had no history of dark urine or hepatitis. She had a more than 30-year history of use of oral contraceptives as treatment of acne vulgaris. In 1980, when she was 16 years old, she used Androcur (cyproterone acetate 50 mg) for nine months in combination with Lynoral (ethinyl oestradiol 0.05 mg). She was treated with 100 mg cyproterone acetate for 10 days and 0.05 mg ethinyl oestradiol for 21 days; the treatment was started on day 5 of the cycle. Afterwards she used several other oral contraceptives such as Diane 35 (cyproterone acetate 2 mg / ethinyl oestradiol 0.035 mg) from 1982 until 1995. Then she used Marvelon (ethinyl oestradiol 0.03 mg/ desogestrel 0.15 mg) for at least one year. At the time of presentation she had been taking Microgynon 30 (ethinyl oestradiol 0.03 mg / levonorgestrel 0.150 mg) since 2001; no other concomitant medication, drugs or alcohol were used. On physical examination no abnormalities were found. The liver was not enlarged. Laboratory studies showed a slightly elevated sedimentation rate and anaemia in the presence of excessive menstrual bleeding. The alkaline phosphatase was 299 U/l (normal 40-120 U/l) and gamma-glutamyltransferase was 120 U/l (normal up to 40 U/l). An ultrasonography of the liver and a computed tomography (CT) scan (64 slice MDCT Philips) (figure 1) showed multiple hypoechoic and hyperechoic lesions. On CT these lesions were from heterogenous densities and were hypodense in the venous phase, suggesting the evidence of multiple hypervascular, possibly metastatic, lesions. PET-CT yielded no evidence of a primary tumour. A liver biopsy was taken at that time and showed occasional dilated sinusoids suggesting peliosis hepatis (figure 2). The biopsy was complicated by a subcapsular liver haematoma and the patient was admitted to hospital. After three days of observation she was discharged. The alkaline phosphatase was raised up to 378 U/l after biopsy, presumably caused by the bleeding. Because of the association of peliosis hepatis with long-term use of oral contraceptives, the Microgynon was stopped. No other cause of peliosis hepatis was likely, because of the 30-year history of use of combined oral contraceptives and no other use of concomitant medication, drugs or alcohol. After two years of follow-up the serum alkaline phosphatase is 173 U/l and gamma-glutamyltransferase is 100 U/l. Regression of the multiple hypervascular lesions has been shown on serial repeated ultrasonography of the liver.
DISCUSSION
Both the epidemiology and natural history of peliosis hepatis are not completely understood. Most patients are asymptomatic and remain undiagnosed or have slowly progressive disease. Peliosis hepatis is often an incidental finding on abdominal imaging, as in our patient. On imaging studies, the differential diagnosis of peliosis hepatis includes other focal liver lesions including adenoma, haemangioma, focal nodular hyperplasia, abscess, hypervascular metastatic lesions, and hepatocellular carcinoma. On CT the lesions usually appear as heterogeneous densities that become hypodense in the late arterial and venous phase. On magnetic resonance imaging (MRI), peliosis hepatis lesions are typically of low signal intensity on T1-weighted images and of high signal on T2-weighted images, with late and slow but intense enhancement on contrast-enhanced T1-weighted images. The first report of generalised peliosis hepatis as a complication of long-term use of oral contraceptives was made by Van Erpecum et al. in 1988.5 The pathogenesis of peliosis hepatis is unclear but probably involves hepatocellular necrosis and injury to the sinusoidal endothelium. However, oral contraceptives do not cause sinusoidal endothelial cell injury, in contrast to other agents such as azathioprine, 6-thioguanine and oxaliplatin. Thus, the mechanism by which oral contraceptives lead to peliosis hepatis remains unclear. Any contributing effect of the earlier use of cyproterone acetate on peliosis hepatis in our patient has not previously been described. Regression of a mild form of peliosis hepatis after discontinuation of an oral contraceptive with resolution of the clinical, laboratory, and radiographic abnormalities is likely. In our patient, generalised peliosis hepatis was discovered during evaluation of abnormal liver enzymes. The diagnosis was not suggested by the various imaging modalities (ultrasonography, PET-CT), but by liver biopsy as earlier reported.6 Biopsy of a suspected lesion established the diagnosis peliosis hepatis in our patient, but gave the complication of major bleeding due to the vascular nature of peliosis hepatis.
CONCLUSION
In the described patient, the diagnosis of peliosis hepatis was not considered before liver biopsy. Peliosis hepatis should be considered in the differential diagnosis of women with a long history of oral contraceptive use with suspected hypervascular lesions diagnosed by imaging but with an unknown primary tumour. Because of the extensive use of oral contraceptives in the general female population worldwide, peliosis hepatis should be added to the differential diagnosis of suspected hypervascular liver lesions in women with a long history of use of oral contraceptives.
REFERENCES