KEYWORDS
Immunocompromised patients; invasive fungal infections; tyrosine kinase inhibitors.
INTRODUCTION
Invasive fungal infections (IFI) usually occur in immunocompromised patients such as patients with acute leukaemia and prolonged neutropenia. Although infections represent an important cause of morbidity in chronic lymphocytic leukaemia (CLL), IFIs are rarely observed. Ibrutinib, a small molecule and potent inhibitor of Bruton’s tyrosine kinase (BTK), was registered for the treatment of CLL in 2014. Since the introduction of BTK inhibitors, the number of CLL patients with IFI has increased. In this article, we describe two patients with CLL who developed an IFI during treatment with a BTK inhibitor.
CASE REPORT
Patient A, a 75-year-old man with CLL in remission using the BTK inhibitor ibrutinib, presented with a painful left forearm. Physical examination showed a pale, sick patient with the clinical signs of cellulitis of his left forearm. Blood tests showed a C-reactive protein (CRP) value of 141 mg/l (reference value: < 10) and increased liver enzymes. A CT scan of the chest and abdomen showed a consolidation in the left upper lobe of the lung and two liver lesions (figure 1a). A percutaneous biopsy of the liver lesions revealed inflammation and the presence of fungal hyphae, which raised the suspicion of disseminated fungal infection. Empirical antibiotic treatment and intravenous liposomal amphotericin-B was initiated (5 mg/kg/day) and ibrutinib therapy was discontinued. Despite the initiated treatment, his upper arm had to be amputated. Molecular analysis on the tissue of the amputated arm showed the presence of DNA from Lichtheimia corymbifera and Aspergillus species. Culture on material obtained from the liver abscess showed hyphae. Combination therapy was initiated by adding posaconazole to the treatment. This combination therapy was continued for one month, after which amphotericin B was discontinued. In the meantime, venetoclax was initiated to treat the CLL. Clinically, the patient recovered and was discharged with improved health. At the time of this writing, 17 months later, he continues to receive posaconazole while the lesions in the liver continue to decrease in size (figure 1b). 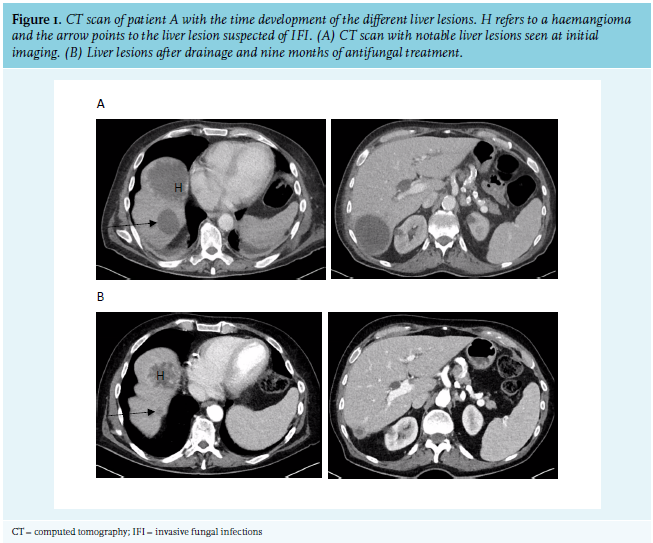
Patient B, a 72-year-old man with atrial fibrillation and CLL in partial remission using ibrutinib, presented himself at the emergency room with symptoms of a cerebrovascular accident. More than a month before presentation at the emergency room, the patient had been started on prednisone (40 mg/day) due to amiodarone-induced hyperthyroidism. Physical examination showed a latent right-sided hemiparesis. Additional blood tests showed no abnormalities apart from a known normocytic anaemia and thrombocytopenia (Hb 6.6 mmol/l; mean corpuscular volume 86 fl; platelets 95 x 109/l) and mild inflammation parameters (CRP 49 mg/l; leukocytes 13.7x109/l). A CT scan of the brain was performed which revealed multiple brain infarctions. Clopidogrel was started in addition to the oral anticoagulation that the patient was already taking for his atrial fibrillation. However, his neurological condition worsened and he developed respiratory distress. Next, an MRI of the brain and CT scan of the thorax was performed which revealed multiple brain abscesses and extensive peribronchovascular consolidations. Suspected of having an IFI, the patient was treated with voriconazole and meropenem. PCR testing of bronchoalveolar lavage fluid confirmed a Serratia marcescens and Aspergillus fumigatus infection. Despite treatment, the patient’s condition soon deteriorated and he died of respiratory failure.
DISCUSSION
CLL is the most common form of leukaemia in adults. New drugs have been developed in recent years, including tyrosine kinase inhibitors such as ibrutinib and acalabrutinib.1-3 Ibrutinib has also been approved for the treatment of other haematological malignancies such as Waldenström’s macroglobulinemia and mantle cell lymphoma. Acalabrutinib is a more selective BTK inhibitor designed to improve the safety and efficacy of first-generation BTK inhibitors such as ibrutinib.3
A recently published observational study showed that IFI occurs more often in CLL patients treated with BTK inhibitors than expected.4 Aspergillus species and cryptococci were most frequently reported. Furthermore, central nervous system involvement was present in a large proportion of these patients (49%) and disseminated infection in multiple organs (60%) was often observed. Interestingly, only a small proportion of patients were neutropenic in the month before the occurrence of the fungal infection (14%).
Why are patients taking a BTK inhibitor at risk of developing IFI? BTK is an intracellular signaling protein that transmits signals from the B-cell receptor (BCR) and is necessary for B-cell survival. Recent preclinical studies have shown that signalling via BTK is also involved in various other processes such as neutrophil attraction, cytokine production, and phagocytosis by macrophages.5-7 Because of these effects on the innate immune system, BTK inhibitors inhibit the effective clearance of fungi that have crossed the patient’s first line of defence. This could explain the risk of IFI when using both non-selective as well as selective BTK inhibitors (i.e., ibrutinib and acalabrutinib, respectively). Indeed, a third case of IFI with Aspergillus species was recently diagnosed by one of the authors of this paper in a patient on acalabrutinib.
The European Organization for Research and Treatment of Cancer (EORTC) and the Mycosis Study Group (MSG) have established guidelines that include risk factors for IFI.8 Use of BTK inhibitors is currently not listed as a risk factor. Despite established guidelines on the diagnosis and management of IFI, the diagnosis remains challenging. Clinical symptoms and radiological findings are often non-specific, especially when a patient is not neutropenic. Moreover, diagnostic tests are not always immediately available in all hospitals. Furthermore, antifungal agents such as voriconazole interact with many other drugs via CYP450 enzyme-mediated metabolism and enzyme inhibition. An additional problem, particularly in the Netherlands, is the development of resistance to antifungal agents of the triazole class as a result of the use of azoles in agriculture.9 Resistance of Aspergillus fumigatus to voriconazole was non-existent in the Netherlands before the year 2000 but has been increasing since then.10,11 This not only complicates treatment but also increases mortality.12,13
CONCLUSIONS
CLL patients treated with BTK inhibitors are at risk of IFI. These infections can be fulminant with serious complications and high mortality, as illustrated by the two cases presented here. Early diagnosis is essential but is hampered by the atypical presentation. Future research is needed to evaluate if certain patient characteristics increase the risk for IFI in patients on BTK inhibitors. If this is the case, antifungal prophylaxis could be considered.
REFERENCES