KEYWORDS
Bleeding, oral anticoagulation, perioperative bridging, post-procedure complications, thromboembolism
INTRODUCTION
Patients with atrial fibrillation (AF), mechanical heart valves (MHV), or venous thromboembolism (VTE) are treated with oral anticoagulation (OAC) for the prevention and treatment of thromboembolism (TE). In patients with AF, OAC reduces the risk of stroke or systemic embolism by 64% and reduces all-cause mortality by 26% compared with no OAC.1 Before 2009, vitamin K antagonists (VKAs) were the only OAC available. Although recently introduced, direct oral anticoagulants (DOACs) are gradually replacing VKA for patients with AF and VTE. The uptake is slow and in 2016, 72% of Dutch patients receiving OAC were still treated with VKA therapy.2
The efficacy of VKA therapy is offset by an increased risk of bleeding. Therefore, invasive procedures including surgery usually require interruption of VKA therapy. Typically, patients are instructed to discontinue VKA treatment three to five days before surgery due to its long half-life. After surgery, adequate anticoagulation is only achieved several days after resuming VKA. This leads to a window of at least five days of subtherapeutic anticoagulation. For patients at high risk of TE, this window can be bridged by an anticoagulant with a shorter half-life, such as low molecular weight heparin (LMWH). This approach may reduce TE, but increases the risk of perioperative bleeding. In practice, perioperative LWMH bridging is used only in patients who have the highest risk of TE. Leading international guidelines on perioperative management of antithrombotic therapy, including the clinical practice guidelines of the American College of Chest Physicians (ACCP, 9th edition, 2012), were mainly based on observational studies and expert opinions.3 These guidelines provide practical guidance for medical professionals, however are not based on high-quality evidence.
Uncertainties regarding perioperative bridging could lead to unnecessary risks for patients and practice variation among medical professionals. In a recent Canadian cross-sectional survey, large practice variation in perioperative anticoagulation management was seen among general internists and haematologists who managed perioperative anticoagulation.4
Recent studies, including the international randomised controlled BRIDGE trial, provided additional evidence and demonstrated that perioperative bridging caused more harm than benefit in most anticoagulated patients with atrial fibrillation.5,6 These studies were instrumental in a more restrictive bridging recommendation in the updated Dutch national guideline in April 2016.7 Local hospital protocols were updated subsequently, often with a time delay.
This retrospective cohort study was performed at a regional hospital and assessed whether bridging practice was already changing after the publication of the updated national guideline, but before adaptation of the local hospital protocol 17 months later. Furthermore, protocol adherence was monitored and TE risk and bleeding risk were compared in bridged and non-bridged patients.
MATERIALS AND METHODS
Study design and patient selection
The retrospective cohort study was carried out at the Jeroen Bosch Hospital (JBH) in ‘s-Hertogenbosch, the Netherlands. Patients were selected from the Thrombosis Service ‘s-Hertogenbosch (TSH), a specialised unit of the hospital dedicated to managing VKA therapy of non-institutionalised patients and patients from regional nursing homes. At TSH, separate, temporary files are kept of patients undergoing elective surgery. TSH is actively involved in preprocedural internationalised normalized ratio (INR) management (see peri-operative protocol below). At the start of our study, files were still available from April 2016. We planned to select patients for a 15- month period.
Patients were included if they were over 18 years of age, used VKA, and had an elective surgical procedure at the JBH with a necessary interruption of their VKA treatment before surgery. Outpatient procedures and surgery at other hospitals than JBH were excluded.
Peri-operative protocol
The ‘Peri-operative anticoagulation management’ protocol of JBH was approved on October 15th, 2010 (first version), with a latest update in April 2014 (the 2014 protocol), which was based on the 2012 ACCP guideline.3 Prior to surgery, the responsible surgeon indicated the bleeding risk of the procedure, whether the VKA therapy should be interrupted (high bleeding risk) or not (low bleeding risk), and the targeted preprocedural INR (below 2.0, below 1.8, or below 1.5). The peri-operative TE risk of a patient was determined during the pre-operative screening by an anaesthesiologist based on the TE risk stratification model used by JBH (table 1). Patients with high TE risk (> 10%) undergoing a high bleeding risk procedures should receive peri-operative bridging. Patients with low (< 5%) or moderate TE risk (5-10%) should not be bridged.
Details of the individual bridging policy per patient were registered in the patient information system by TSH. The VKA therapy (acenocoumarol and phenprocoumon) should be interrupted two to four days prior to surgery depending on the target INR as determined by the responsible surgeon. Additional vitamin K was allowed in cases where phenprocoumon was used. LMWH therapy was started at the same time and stopped 24 hours before the procedure. The VKA and LMWH therapy were restarted 12 to 24 hours post-procedure, except in cases of an active bleeding, to be decided on by the responsible surgeon.
In 2017, the 2014 protocol was updated by the antithrombotic taskforce of JBH based on the Dutch national guideline of 20167 and resulted in an adjusted protocol in August 2017 (The 2017 protocol). Although ready to be implemented in April 2017, final board approval was delayed until August 2017 due to administrative reasons.
Differences between the 2014 protocol and the 2017 protocol in terms of TE risk stratification are presented in table 1. In both protocols, perioperative bridging was advised in patients with high TE risk (> 10%).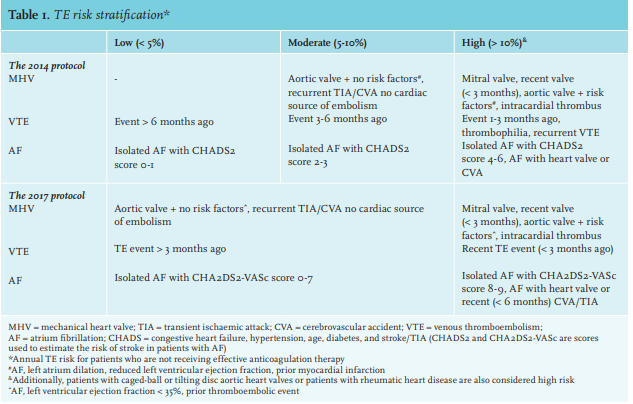
Reporting period
The total reporting period was divided into subperiods to facilitate analyses over time. Two equal six-month periods were selected, during which the JBH 2014 bridging protocol was in place (April-September 2016 and October 2016-March 2017). A third three-month period (April 2017-June 2017) was added to reflect the interim period between the 2014 protocol and the 2017 protocol. Although the 2017 protocol was not officially adopted until August 2017, it might have had an influence on bridging decisions and behaviour in the period from April 2017 to June 2017.
File review
A standardised electronic questionnaire was prepared to structure and to facilitate patients’ file review and data analyses. Patient files were reviewed in the JBH electronic patient information system. This database-oriented computer system was introduced at JBH in June 2016. Files of the previous computer system were converted into the database. If necessary, data was completed with information from the TSH information system. Patients were stratified according to their risk of perioperative TE based on patients’ clinical indication for anticoagulation and the presence of comorbidities (see table 1).
Outcome variables
In the present, study bridging was defined as the administration of a therapeutic dose of subcutaneous LMWH or intravenous unfractionated heparin (UFH) for a short period of time during interruption of VKA therapy when the international normalized ratio (INR) was below therapeutic range (INR < 2.0). This includes both full bridging (pre- and post-procedure) and post-procedural bridging only. The outcomes were the proportions of patients receiving bridging, adherence to hospital protocol, and the incidence of post-procedural TE or bleeding (major bleeding or clinically relevant non-major bleeding). TE events were defined as either arterial (ischaemic stroke or transient ischaemic attack) or venous (pulmonary embolism or deep vein thrombosis) as documented by appropriate imaging techniques. The primary bleeding outcome was the composite of major and clinically relevant non-major bleeding. Major bleeding was defined as bleeding which is fatal, occurs in a critical organ, causes a haemoglobin (Hb) drop of at least 1.25 mmol/l, or requires transfusion of two or more units of packed red blood cells. Clinically relevant non-major bleeding was defined as bleeding that did not qualify as major, but required medical intervention, advise of a physician, pharmacological intervention, were registered in the patient’s file, or caused discomfort for the patient. Intraoperative bleeding or Hb drop due to dilution by intra-operative fluid administration were not qualified as bleeding. TE events and bleeding were included up till 30 days after the surgical procedure.
Statistical analyses
Categorical variables were presented as absolute numbers and proportions; and continuous variables as means and standard deviations or median and interquartile range, according to the normality of the data. All the analyses were conducted using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp, Armonk, NY). Differences between categorical variables were evaluated by Chi square tests or similar tests. A p-value below 0.05 was considered statistically significant. In order to evaluate the impact of perioperative bridging on bleeding, the odds ratio for bleeding between patients treated with bridging and patients without bridging was calculated with a 95% confidence interval. Logistic regression analysis was performed to identify possible confounders for the association between bridging and bleeding. This regression analysis was focused on variables such as prior stroke, abdominal surgery, and type of anticoagulation. Variables would be qualified as confounders if the impact of the odds ratio was more than 10% between LMWH bridging and bleeding.
RESULTS
Patients
From the 488 patients in the TSH files during the period of April 2016 to June 2017, 98 patients (20%) were excluded at the beginning of the study due to cancelled or postponed surgery or VKA continuation during procedures, such as percutaneous transluminal angioplasty or cataract surgery. As a result, 390 patients were available for the analysis.
Patient characteristics are shown in table 2. Mean age was 72.7 years with 64% of patients being male. The indication for VKA therapy was AF in 79% of patients, VTE in 10% of patients, MHV in 5% of patients, and 6% for other indications. The mean CHADS2 score of AF patients was 2.0. Just over 93% of patients in this study used acenocoumarol as VKA, the remainder phenprocoumon. The mean pre-procedure INR of 1.21 was well below the average targeted INR of 1.79.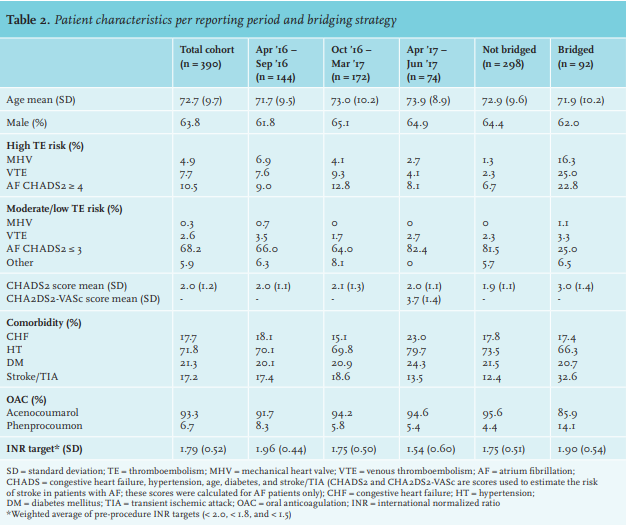
Surgical procedures
Orthopaedic procedures were most prevalent (25.4%), followed by urological (19.2%) and abdominal (18.5%) surgery. Plastic and vascular surgery each comprised 11.8% of procedures. All interventions were considered high bleeding risk procedures based on the 2014 protocol. Figure 1 shows the categories of surgical procedures over the reporting period.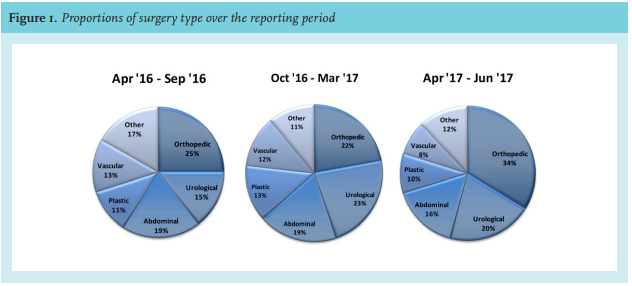
Bridging strategy over time
LMWH bridging was used in 24% of patients undergoing surgery. In total, 92 patients were bridged, with 61 patients (66%) receiving pre- and post-operative bridging whereas 31 patients (34%) only received post-procedural bridging. The proportion of bridged patients over the total reporting period decreased from 27% in the period April to September 2016 to 23% in the period October 2016 to March 2017, and further to 18% in the period from April to June 2017.
In high TE risk patients, the average bridging rate over the total reporting period was 66% (79% in MHV patients, 77% in VTE patients, and 51% in AF patients). The proportion of high risk TE patients with VTE or AF that received bridging therapy decreased from 91% and 77% respectively in the first period to 33% in the last period. In high risk patients with mechanical heart valves, the bridging rate remained stable at 70-80% in the first 12 months and increased to 100% at the end of the reporting period (figure 2).
In low and moderate TE risk patients, the average bridging rate was stable at 10-13% over the reporting period. In patients with MHV, VTE, and other VKA indications, the bridging rate decreased to 0% at the end of the reporting period. In patients with AF, the bridging rate increased over the reporting period from 5% to 13% due to more post-procedural bedside bridging decisions (see figure 3). For the analyses of temporal trends in LMWH bridging, the reporting period was divided into two six-month periods and one three-month period. To evaluate whether this breakdown influenced the results, an alternative analysis was done with three periods of five months, which yielded similar results.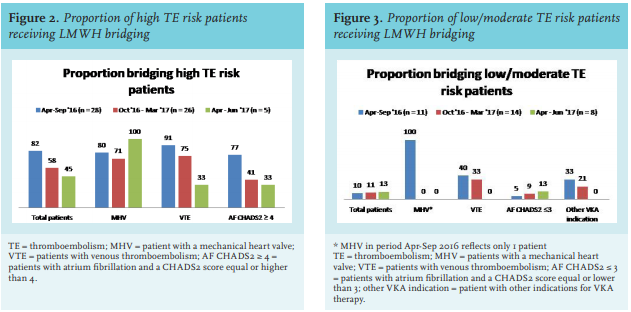
Adherence to protocol and the 2016 Dutch national guideline
Over the reporting period, adherence to the 2014 protocol for high TE risk patients decreased from 80% (April 2016 to September 2016) to 56% (October 2016 – March 2017) and to 43% (April 2017 – June 2017; figure 4). For low and moderate risk patients, protocol adherence was stable around 90%. Concomitantly, we observed that patients were managed according to the new national guideline published in April 2016 before the adaptation of the local hospital protocol was implemented. Adherence to this new guideline in non-bridged patients was 99.3% over the total reporting period (April-September 2016: 100%; October 2016-March 2017: 98.5%; April-June 2017: 100%) (see table 3).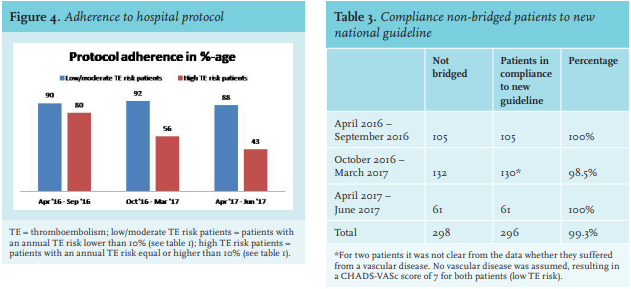
TE events 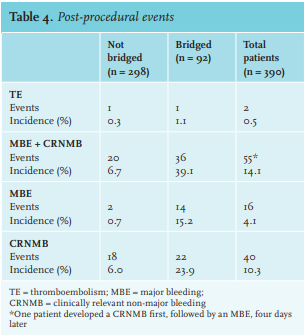
Two patients developed a suspected TIA in the 30 days following the procedure (incidence 0.5%). The events occurred in patients with AF at 1 and 14 days after the procedure. Both patients were at high risk of TE based on the hospital protocol (AF, CHADS2 score 4 and 5, respectively). One patient (with TE event one day post-procedure) did not receive bridging. VKA therapy was interrupted four days prior to surgery and restarted the day after the procedure. The other patient received bridging with LMWH. VKA therapy was interrupted three days prior to the procedure and restarted one day post-procedure (table 4).
Bleeding events
In total, 55 patients (14.1%) had a bleeding episode (major or clinically relevant non-major bleeding) within 30 days after the procedure. The risk was higher in patients treated with LMWH bridging than in non-bridged patients (39.1% vs 6.7%, odds ratio 8.5, 95% confidence interval 4.6-15.8). Sixteen patients (4.1%) developed a major bleeding within 30 days after the procedure. Major bleeding occurred most often in abdominal surgery (11.1%, 8 events), followed by gynaecological surgery (10.0%, 1 event) and breast surgery (7.7%, 1 event) (table 4).
Logistic regression was performed to identify possible confounders. Unfortunately, the low number of observations of major bleeding did not allow for separate logistic regression. For this reason, regression has been extended to the impact of confounders on major and clinically relevant non-major bleeding taken together. No confounders were identified.
DISCUSSION
In recent years, practice guidelines on perioperative management of VKA therapy have recommended more restrictive use of LMWH bridging in patients who require temporary interruption for surgical procedures.7 This change was caused by evidence from a randomised trial that confirmed previous observational studies that LMWH bridging in patients with atrial fibrillation increases the risk of post-operative bleeding without protecting against thromboembolic events.5,8 In the present study, adherence to the hospital bridging protocol dropped from 80% to 43% in 15 months for patients at high TE risk and remained high (~ 90%) for intermediate and low TE risk procedures. This steep decline was brought on by the new Dutch national guideline on perioperative VKA therapy in April 2016. Although the hospital protocol was not changed until August 2017, clinical practice had already started to change after publication of the national guideline. This raises an important issue on the necessity of local hospital protocols on topics for which national multidisciplinary guidelines are available. If guidelines are drafted by mandated representatives of the involved specialties, local evaluation and translation into a new hospital protocol may not be necessary, which only delays implementation of recommendations to improve patient outcome. This study shows that physicians may already start to adopt new guidelines before hospital protocols are adapted. On the other hand, guidelines often offer multiple options in circumstances where evidence is less clear and guidelines usually lack details that a hospital protocol requires, such as drugs names, recommended dosage, or frequency. A hybrid approach that does not re-evaluate the evidence but does make explicit choices may reduce the time and effort needed to update local protocols. We could not compare adherence to hospital protocol at our institution with other hospitals and do not know of such available data. We speculate however, that a similar pattern would have been witnessed in other hospitals.
In this study, LMWH bridging increased the risk of bleeding and did not reduce perioperative thromboembolism in the reporting period. Although this is in agreement with previous studies, the present study was not powered to study differences in bleeding and thromboembolism in bridged versus non-bridged patients. Other limitations involve the retrospective nature of the study. Patient information was extracted by review of TSH charts, which are semi-structured and some details were unclear or may have been missing. Furthermore, due to the introduction of a new electronic record in July 2016, available information for the period April-June 2016 was limited.
CONCLUSION
In conclusion, this study indicates that in daily practice, physicians already adopt new evidence from guidelines before local hospital protocols are changed accordingly. It also confirms the rationale for a more restrictive LMWH bridging approach in patients on VKA therapy who need to interrupt oral anticoagulation for surgery.
DISCLOSURES
This study did not receive any financial support. G.C.M. Mol, H.A.M. Sinnige, and N.C.V. Péquériaux report no conflicts of interest for this study. H.R. Büller has served as a consultant to Sanofi-Aventis, Bayer, Pfizer, Glaxo-Smith-Kline, Astellas, Boehringer-Ingelheim, and Daiichi-Sankyo, outside of the submitted work. M. Coppens has received financial support for research and health innovation, as well as lecturing and consultancy fees from Bayer, Boehringer Ingelheim, Bristol Myers-Squibb, Daiichi Sankyo, Pfizer, Portola, and Sanquin Blood Supply, outside of the submitted work.
REFERENCES