KEYWORDS
Rheumatoid arthritis, nutritional and metabolic diseases, cardiovascular diseases, disease activity, metabolic syndrome
INTRODUCTION
Rheumatoid arthritis (RA) is a systemic auto-inflammatory disease with chronic joint damage and disability. Early diagnosis and proper treatment are the key factors for treatment success.1 Cardiovascular disease (CVD) is the most commonly identified cause of death in RA.2 In RA patients, metabolic features may be altered. These alterations may be the underlying mechanisms of increased CVD rate. Body composition changes, increased insulin resistancy, alterations in lipid parameters and adipokine levels would be the most significant impairments related to RA. Herein, some of these changes may also be seen in metabolic syndrome (metS).3
Not only traditional CVD risk factors, but also systemic inflammation may account for increased frequency of CVD events in RA.4 Lipid parameters may change in both a quantitative and qualitative manner during inflammatory conditions. Furthermore, more atherogenic sub-fractions were highlighted during the disease.5 These changes in lipid parameters are termed as lipid paradox. Metabolic alterations during active disease, including paradoxical changes in lipid profile, could increase the risk of cardiovascular mortality.
It is known that metabolic changes may be seen even in preclinical RA. Also, during the course of the disease, especially in cases with high disease activity, metabolic changes may be more significant.6 Therefore, the European League Against Rheumatism (EULAR) task force recommends both controlling disease activity and treating traditional CVD risk factors together for preventing disease-related disability and lowering CVD risk.7
MetS may be more frequent in patients with RA. Furthermore, it was found that throughout the disease course, overall risk for developing metS was higher in RA patients when compared to healthy controls.8 So, detection of metabolic disorders at early stages of the disease along with effective disease activity control may reduce the risk of CVD.9 It is also known that like full-blown metS, every particular metabolic alteration in metS might be associated with CVD related mortality.10 Therefore, evaluating and treating every particular metabolic alteration may also be significant for lowering CVD risk in RA.
Glucocorticoids are usually used in the management of RA; however they may also contribute to the increased risk of metS. Furthermore, other disease-modifying treatments may also have effect on metS frequency. To ourknowledge, there has not been a study in the literature that evaluated the features of metS in treatment-naïve RA patients even before starting any disease-modifying anti-rheumatic drugs (DMARD) treatment. In this study, we examined the hypothesis that metS is more frequent in treatment-naïve RA patients than controls without inflammatory diseases, even before starting any DMARD treatment. Therefore, we could exclude the interference of standard DMARD treatment (including glucocorticoids) on metabolic and anthropometric components. Then, we compared the frequency of metS-related metabolic and anthropometric alterations between RA patients and healthy controls. Lastly, we evaluated the differences of disease-related parameters between the RA patients with or without metS.
MATERIAL AND METHODS
The study was performed in Kartal Dr. Lutfi Kirdar Training and Research Hospital between the dates of January 2017 to January 2018. We enrolled 53 patients with RA who fulfilled the 2010 American College of Rheumatology/EULAR RA Classification Criteria.11 All patients were diagnosed with RA for the first time in our outpatient rheumatology clinic. None of the patients had received any treatment, including glucocorticoids due to their symptoms. All consecutive newly diagnosed RA patients accepted to enrol in the study. At the same time, we enrolled 55 age- and sex-matched subjects as a control group from the same outpatient clinic. None of the controls were previously diagnosed for rheumatologic diseases. Moreover, all of the controls presented at the hospital with the complaints of non-specific symptoms including arthralgia, non-specific pain, and constitutional symptoms. None of the subjects in control group had any pathologic findings in their physical examination. Likewise, none had increased acute phase reactants or positive serologic tests. For control group selection, we appointed 504 subjects as possible controls between the dates of January 2017 to January 2018. Then, we randomly enrolled 55 ageand sex-matched subjects as control group from among those 504 subjects. In this study, we diagnosed patients and controls as metS using 2001 Adult Treatment Panel III report (ATP III)-defined criteria for the metabolic syndrome.12
RA related features
RA patients were evaluated for duration between RA-related symptoms onset to diagnosis, visual analogue scale (patient global health), number of tender and swollen joints, rheumatoid factor (RF), anti-citrullinated protein antibody (ACPA), sedimentation rate, C-reactive protein (CRP), and disease activity. We measured disease activity with disease activity score 28 joint C-reactive protein (DAS28-CRP).13
Metabolic and anthropometric components
All study participants were evaluated for medical history of diabetes mellitus (DM), hypertension (HT), and coronary heart disease; metabolic parameters included triglycerides, total cholesterol, high density lipoprotein cholesterol (HDL), low density lipoprotein cholesterol (LDL), fasting glucose; anthropometric parameters included waist circumference, hip circumference, height and weight, and lastly systolic and diastolic blood pressure measurements. Blood pressure was measured in sitting position after 30 minutes of rest in a quiet environment using a mercury sphygmomanometer. Body mass index (BMI) was calculated as previously shown.14 All anthropometric parameters measured according to Centers for Disease Control and Prevention Anthropometry Procedures Manual.15 This study was approved by the Local Research Ethics Committee and carried out in compliance with the Helsinki Declaration. All the patients gave written informed consent.
Statistical analyses
Statistical analyses were carried out using SPSS Version 17.0 (SPSS Inc., Chicago, IL, USA). In order to determine if the data were normally distributed, the Kolmogorov-Smirnov test was performed. All continuous variables distributed non-normally. The comparisons of the continuous variables between patients were performed by the Mann-Whitney U test. Moreover, comparisons of the categorical variables were implemented by Chi-square test. Cut off values for HDL, and hip and waist circumferences have gender differences for fulfilling ATP III criteria. Therefore, we compared these parameters for different genders separately. First, we compared the metS frequency, and metabolic and anthropometric parameters between RA and controls. Then, the RA patients were sub-divided into two groups according to fulfilling ATP III criteria as those with metS and without metS.12 Disease-related parameters were compared between these groups. The results are given as median (interquartile range). We performed Bonferroni correction for protecting type 1 error. In our study, we compared 35 different variables between the groups. Therefore, after correction, p ≤ 0.001 was considered as statistically significant.
RESULTS
Demographic and disease-related features of the study participants
In both groups, male:female ratio was 1:3.5. The median age in both groups was 51.0 years. Furthermore, the median duration between symptom onset to diagnosis was 6.0 (2.25-14.2) months. Herein, 32/53 (60.3%) of the patients were diagnosed as RA within six months of symptom onset. Anti-citrullinated protein antibodies (ACPA) were positive in 25/53 (47.1%) of the patients. The median DAS28-CRP score of the patients was 5.3 (4.1-5.2).
Metabolic and anthropometric features of the study participants
The number of subjects with metS were 25/53 (47.1%) in the RA group and 9/55 (16.4%) in controls. MetS was found statistically more frequent in RA patients than controls (p = 0.001; OR, 4.56; CL%95 1.86-11.16). All anthropometric parameters were similar in both groups. Likewise, there were no statistically significant differences between groups according to lipid parameters. However, total cholesterol, and LDL and HDL levels were lower (but not significantly so) in RA patients as compared to controls. Furthermore, systolic and diastolic blood pressures, fasting glucose levels, and DM, HT, CVS disease frequencies were similar in both groups. There were five different components in ATP III criteria for metS. The only component with different frequency between RA and controls was fasting glucose/ established DM item. The number of patients who fulfilled this particular criteria item was higher in RA patients (p < 0.001). RA patients fulfilled three of the remaining four components more frequently than the control group. However, these differences were not statistically significant. Herein, controls fulfilled the triglyceride item more frequently than RA patients. Additionally, RA patients fulfilled significantly higher number of particular criteria components as compared to controls (p < 0.001) (table 1).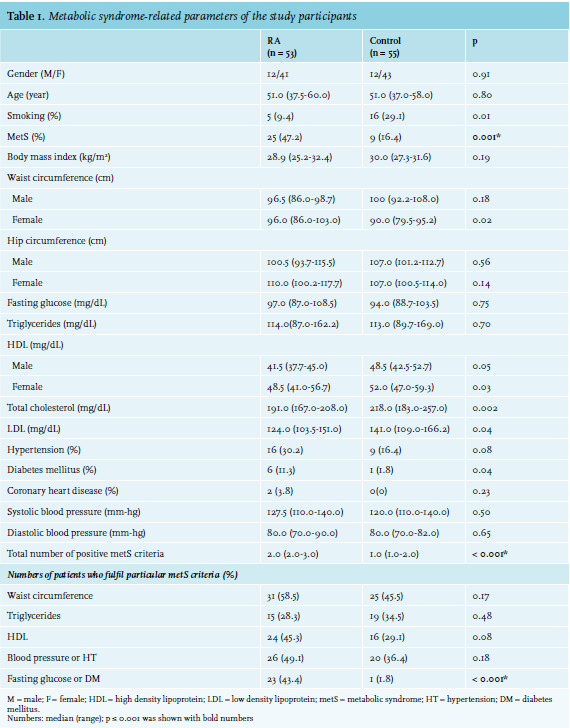
Demographic and disease-related parameters between patients with or without metS
Demographic features, disease activity, frequency of sero-positivity, and duration between symptom onset to diagnosis were similar between the patients with or without metS. However, disease activity was non significantly higher in the patients with metabolic syndrome. Furthermore, patients with metS were older. Nevertheless, this difference was not statistically meaningful (table 2).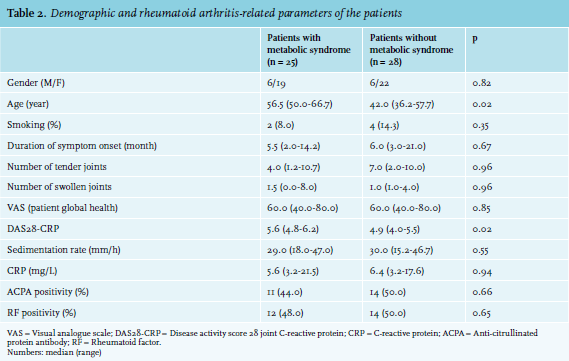
DISCUSSION
In our study, we showed that metS frequency in treatment-naïve, newly diagnosed RA patients was higher than the controls from the same outpatient clinic without inflammatory diseases. All anthropometric and metabolic parameter were similar in both RA patients and controls. However, HDL, total cholesterol, and LDL levels were not significantly lower in treatment-naïve RA patients than controls. Furthermore, the numbers of patients who fulfilled fasting glucose/established DM item were significantly higher in treatment-naïve RA patients. Our study is unique because most of the patients had early RA. Additionally, unlike other early RA cohorts, none of our patients had been previously treated.
MetS frequency in early RA patients was previously found between 16-31% depending on the criteria used for diagnosing metS.6 In our study, 47.1% of the treatment-naïve RA patients fulfilled the ATP III metS criteria. This was statistically higher than metS frequency in our control group from the same outpatient clinic without inflammatory diseases (16.4%). Furthermore, 33.9% of the Turkish background population was diagnosed as metS according to a nationwide study.16 Accordingly, these results might have showed that even in early, treatment-naïve and newly diagnosed RA patients, the frequency of metS would be higher than in the normal population. Likewise, it was shown that leptin/adiponectin ratio may increase even at the pre-RA stage. Increased inflammatory cytokines during active disease is thought to be responsible for increased leptin/adiponectin ratio.17 Therefore, increasing levels of pro-inflammatory and pro-atherogenic adipokines and cytokines may relate to higher frequency of metS in early and treatment-naïve RA patients.
In our study, RA patients had lower HDL, LDL, and total cholesterol levels compared to controls. All differences were found non-significant after Bonferonni correction. However, our results may show tendency to lower cholesterol levels in treatment-naïve, newly diagnosed RA patients. HDL, LDL, and total cholesterol levels usually reduced depenent upon inflammation.18 Lipid profile alterations in our study were also concordant with previous studies in RA patients.19,20 As shown previously, decreased HDL, LDL, and total cholesterol levels have been accepted as CVD risk factors in RA patients.3,21 Suppressing inflammation with synthetic or biological disease-modifying drugs (DMDs) may paradoxically increase the LDL and total cholesterol levels.20 But, contrary to expectations, these metabolic effects of the DMDs lowers the risk of CVD.22 Other than quantitative lipid changes, RA patients may have pro-atherogenic structural and functional changes in lipid sub-fractions. These changes may also be the reason for increasing CVD in RA. During active disease, even with low levels of LDL and total cholesterol, the frequency of CVD increases.5 Here, HDL particles become less protective against atherosclerosis. Moreover, LDL particles become more oxidised and atherogenic.5,23 Therefore, according to our results, as expected in an active disease state, newly diagnosed and treatment-naïve RA patients may have a tendency towards atherogenic lipid level alterations. All of these alterations were independent of the influence of DMDs.
Previous studies showed that RA patients had increased waist circumference, elevated blood pressure, and high fasting glucose levels compared to the healthy population.6 Also, in an early RA cohort, high BMI and increased disease activity were found to be associated with metS.24 We found that BMI of our patients and controls were similar.25 In our study, we demonstrated that all anthropometric parameters were similar between the patients and controls. Furthermore, 23/53 (43.4%) of the patients compared to 1/55 (1.8%) of the controls fulfilled metS criteria for fasting glucose/DM, and both fasting glucose levels and DM frequency were similar between the groups. However, there was a tendency for higher fasting glucose levels in RA patients compared to controls, and DM frequency was non-significantly higher in patients than controls. It was shown that insulin resistance increases in RA patients.26 Moreover, during high disease activity, pancreas beta-cell activity usually reduces.25 In our study, we did not evaluate insulin sensitivity. Therefore, we could only speculate that increased insulin resistance may also be found in treatment-naïve RA patients. This may explain the alterations in glucose parameters.
The frequency of metS was increased, in particular, in established RA patients with higher disease activity.27,28 In our study, new diagnosed patients with metS had higher disease activity compared to the non-metS group. However, this difference was not significant after Bonferroni correction. Tumour necrosis factor may be increased during active inflammatory states. Both high inflammatory conditions and high tumour necrosis factor levels may alter body mass, lipid, and adipokine profiles. Even though rheumatoid cachexia is more frequent in uncontrolled RA, visceral fat mass may increases during active disease. It was found that visceral fat mass is associated with hypertension, higher fasting glucose, and metabolic syndrome.29
This study had some limitations. First, a limited number of patients was enrolled to the study; however, all patients were treatment-naïve and newly diagnosed. Second, we did not evaluate the pathophysiological aspects of the actual metabolic alteration that we illustrated in the study. These included insulin sensitivity, levels of adipokines, and pro-inflammatory cytokines. Therefore, we could only speculate how these metabolic changes would have emerged. Lastly, even though both metabolic and anthropometric components were similar between the groups, we found a metS more frequently in RA patients than controls. This may be because we diagnosed metS with by individual patient’s performance with criteria and performed conservative statistical methods for comparing variables. Therefore, it would be harder to demonstrate significance of the differences with this method.
In conclusion, the frequency of metS in new diagnosed RA patients was higher than in controls without inflammatory diseases from the same outpatient clinic. Additionally, there were a tendency towards atherogenic lipid changes in treatment-naïve RA patients. Therefore, evaluating metabolic alterations since the diagnosis, controlling the disease activity, and treating metabolic alterations along with standard disease-modifying therapy may be the first steps for reducing CVD risk in RA patients.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES