KEY WORDS 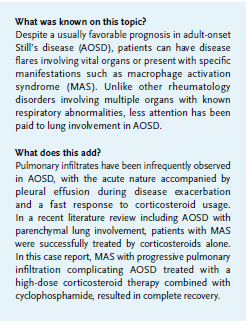
Adult-onset Still’s disease, AOSD, macrophage activation syndrome, pulmonary involvement
INTRODUCTION
Adult-onset Still’s disease (AOSD) was first reported in 1971 by Eric Bywaters in 14 adult patients who failed to fulfill the criteria of classic rheumatoid arthritis.1 It is a rare systemic auto-inflammatory disorder with high spiking fever, evanescent skin rash, arthralgia/arthritis, neutrophilic leukocytosis and marked hyperferritinemia.2,3 Despite a usually favorable prognosis in AOSD, patients can experience disease flares which involve vital organs, or present specific clinical features, such as macrophage activation syndrome (MAS).4 Here, we report on an AOSD patient with MAS-related pulmonary parenchymal involvement who was successfully managed by high-dose corticosteroids and pulse cyclophosphamide therapy.
CASE REPORT
A 19-year-old Han Chinese female was presented with polyarthritis affecting her wrists, knees and ankles, and a recurrent maculopapular erythematous rash over her trunk and limbs during febrile spikes (above 390C). Laboratory tests revealed leukocytosis (10,600 to 15,800/µl) with dominant neutrophil classification (82 to 92%), elevated liver enzyme levels, absence of autoantibody profiles and negative microbiological examinations. One year later, she visited the outpatient rheumatology clinic with a series of clinical, laboratory and radiological surveys, leading to the diagnosis of AOSD by exclusion of infection, malignancy or other rheumatologic diseases. 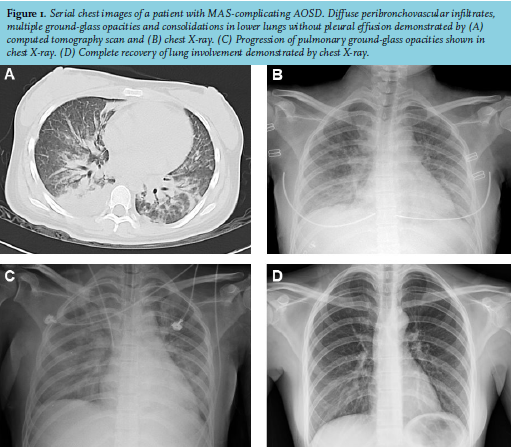
She was brought to the emergency department one month later due to a cough and dyspnea, where radiological images demonstrated diffuse peribronchovascular infiltrates, multiple ground-glass opacities and consolidations in her lower lungs without pleural effusion (figures 1A and B), as well as hepatosplenomegaly. Hemogram was hemoglobin = 8.0 g/dl, platelet count = 25,000/µl and leukocyte count = 9,300/µl (neutrophils 63%), and bone marrow examination revealed hemophagocytosis. She exhibited elevated levels of aspartate aminotransferase (1,115 U/l), alanine aminotransferase (311 U/l), ferritin (9,655 ng/mL), triglycerides (388 mg/dl) and impaired estimated glomerular filtration rate (22 ml/min/1.73 m2 ) with unremarkable urinalysis. Pathogenic microorganisms were not isolated despite extensive cultures. MAS complication was identified with the prescription of methylprednisolone 20 mg, every eight hours by injection. However, bloody sputum with a significant drop of hemoglobin led to a suspicion of diffuse alveolar hemorrhage. Multiple petechiae and hematuria with global coagulation tests fulfilled the disseminated intravascular coagulation criteria, followed by attacks of generalized tonic-clonic seizure; both are distinct AOSD-related MAS presentations.4 A monthly pulse cyclophosphamide 750 mg infusion was initiated due to progressive pulmonary infiltration (figure 1C) and persistent multi-organ abnormalities. The patient had a complete recovery of lung involvement (figure 1D) and other systemic dysfunction with daily corticosteroids replaced by weekly methotrexate therapy during outpatient follow-up.
DISCUSSION
Unlike other rheumatology disorders involving multiple organs with known respiratory abnormalities, little attention has been paid to lung involvement in AOSD.5 By excluding the infectious etiology, pulmonary infiltrates have been observed in fewer than one-tenth of AOSD patients, with its acute nature accompanied by pleural effusion during disease exacerbation and a fast response to corticosteroids usage.6 In a recent literature review including 18 AOSD cases with parenchymal lung involvement, two with MAS were successfully managed by corticosteroids alone.7 In another review with nine cases of corticosteroid-resistant AOSD-associated MAS significant responses were observed in all 5 patients receiving cyclophosphamide injection, despite no associated pulmonary parenchymal involvement.8 In the reported patient with progressive pulmonary infiltration under the high-dose corticosteroid therapy, adding cyclophosphamide resulted in complete recovery. Notably, biologics have proven to be safe and effective in the long-term management of AOSD, particularly in cases with systemic involvement.9 Since MAS is characterized by a cytokine storm with overproduction of pro-inflammatory cytokines, anti-cytokine agents are an attractive approach in treating this complication.10 Indeed, in young female victims, cytokine blockades as alternative therapeutics can avoid the well-known cyclophosphamide-related gonadal toxicity.
DISCLOSURES
All authors declare no conflict of interest. There was no funding or financial support in this report.
REFERENCES