KEYWORDS
Free thyroxine, thyroid, thyroid dysfunction, thyroidstimulating hormone
INTRODUCTION
Thyroid function tests may show a combination of a normal concentration of serum thyroid-stimulating hormone (TSH) and an increased or decreased concentration of serum free thyroxine (free T4).1-4 Often hyperthyroxinemia or hypothyroxinemia in combination with a normal TSH has limited clinical relevance, for example when it is caused by changes in T4-protein binding due to certain medication.5 On the other hand, a normal TSH and aberrant free T4 can reflect a serious underlying condition such as a pituitary disorder. The current literature is unclear about the frequency of the occurrence of hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH and there is discussion about how it should be addressed. Follow-up can possibly be improved when physicians have more knowledge about its probable causes in every day practice. The aim of this study was to determine the 5 year prevalence of a normal TSH in combination with an aberant free T4. Furthermore, this study tried to determine whether any causative factors could be established by the treating physician and whether the treating physician ordered any further diagnostic tests or initiated any treatment. We also checked the medical files ourselves for any identifiable factors, even if no cause was recorded by the treating physician.
Table 1 gives an overview of the many medications and conditions that can cause the combination of hyper thyroxinemia or hypothyroxinemia and a normal TSH. 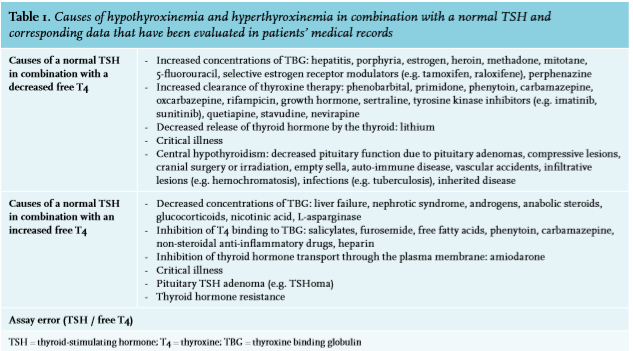
MATERIALS AND METHODS
Study design and settings
A retrospective cohort study was performed at Alrijne Hospital, Leiderdorp, the Netherlands, a non-university general hospital situated in an urban area. Alrijne Hospital has 440 staffed beds, 18,000-20,000 admitted patients per year and around 126,000 new outpatient visits per year.6
Patients
Eligibility criteria included all patients aged 18 years and older who were seen by any kind of medical specialty as either an in- or outpatient, between 1 January 2010 and 31 December 2014.
Patients were included if laboratory results showed an aberrant free T4 in combination with a normal TSH.
Patients were excluded if they used thyroid hormone replacement (for example levothyroxine and liothyronine) or thyroid inhibitory medication (for example propylthiouracil and thiamazole), had undergone thyroid surgery or had been treated with radioactive iodine in the last 2 months, and if they were pregnant. Patients without any notes in their medical file were excluded as well.
Assays
Prior to 13 May 2014 concentrations of free T4 and TSH were determined by a Siemens Immulite 1000 immuno-assay analyser. Maximal total coefficients of variation for free T4 and TSH were 12.1% and 17.5%. Reference values of free T4 and TSH were 10.3-24.5 pmol/l and 0.4-4.0 mU/l. As of 13 May 2014 the laboratory used a chemiluminescent microparticle immunoassay (CMIA; Architect, Abbott Diagnostics USA). The Abbot assay has a dilution factor of 75 before measuring FT4. Maximal total coefficients of variation were 7.8% and 5.3% for free T4 and TSH respectively. Reference values of free T4 and TSH were 10-19 pmol/l and 0.27-4.2 mU/l, respectively. Concentrations outside the reference range were considered abnormal.
Data collecting
The institution’s computerized laboratory information system was used to identify all patients with a normal TSH in combination with an aberrant free T4 between 1 January 2010 and 31 December 2014. The medical records of these patients were retrieved and evaluated for general data, such as age at which the aberrant value was determined, sex, length, weight, body mass index, TSH, free T4, free T3, total T4, total T3, anti-thyroid peroxidase antibodies (anti-TPO), anti-thyroglobulin antibodies (anti-TG) and anti-TSH-receptor (anti-TSH-R). We evaluated recorded causes of hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH and looked into whether the treating physician ordered any tests to examine possible causes. We also checked ourselves if we could identify a cause for the aberrant combinations of free T4 and TSH, even if no cause was recorded by the treating physician. Furthermore we determined if the treating physician started treatment or arranged for some other follow-up.
Medical Ethical Committee
The Medical Ethical Committee of Alrijne Hospital granted permission to perform a medical record study.
RESULTS
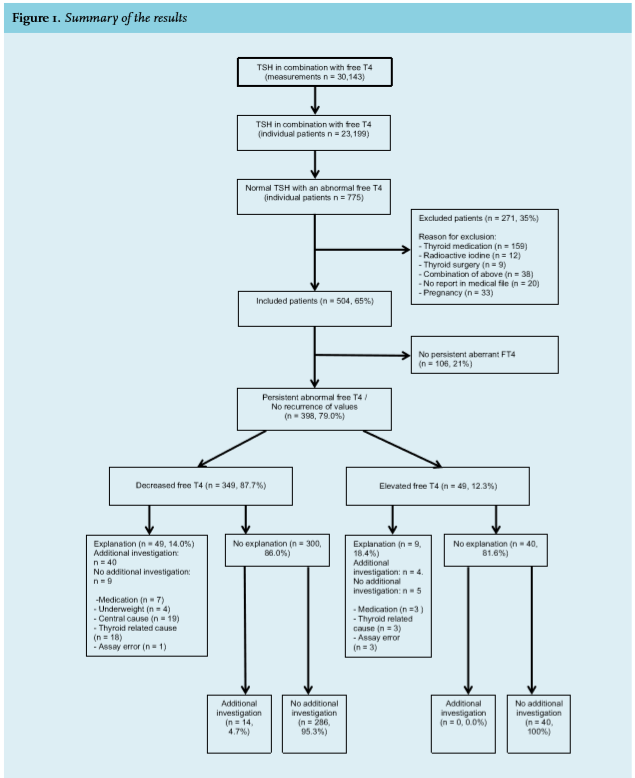
Using the exclusion criteria, out of a total of 775 patients 271 patients (35%) were excluded from this study and 504 patients (65%) were included.
During the 5-year study period, 37,331 TSH tests were performed in 30,143 cases, of which free T4 was measured as well, reflecting 23,199 individual patients. The combination of a normal TSH with an aberrant free T4 was identified 1005 times in 775 individuals (prevalence 334 per 10.000). 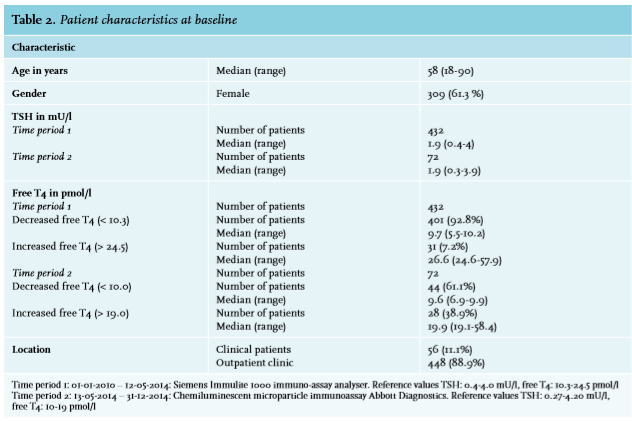
Descriptive characteristics of the study population are shown in table 2. In the table we divided the study period into 2 separate time frames: the period when the Siemens Immulite 1000 immuno-assay analyser has been used and the period when the Abbot assay has been used.
Most patients were seen by an internist (37.9%) or a cardiologist (32.3%).
Of the 504 patients included, 398 had a persistent aberrant free T4. In 106 patients (21%) the aberrant free T4 concentrations did not persist: in 88 patients (83%) free T4 concentrations normalized without any form of intervention, whereas in other patients TSH concentrations became aberrant, also without any intervention.
In 349 (87.7%) of the 398 patients with a persistent aberrant free T4, free T4 was decreased in combination with a normal TSH, 49 patients (12.3%) had an increased free T4 in combination with a normal TSH.
No explanation for the aberrant values was found in 300 of the 349 patients (86.0%) who had a decreased free T4 in combination with a normal TSH. No additional investigation had been carried out in most of these 300 cases (286 patients, 95.3%) and for none of them thyroid hormone replacement had been prescribed. Additional investigation had been performed for the remaining 14 (4.7%) patients, but no explanation for the aberrant values had been found. Seven (50%) of these patients had been prescribed thyroid hormone replacement.
In 49 cases (14%) an explanation for the decreased free T4 in combination with a normal TSH was identified by the treating physician: medication (lithium, amiodarone, venlafaxine, carbamazepine), underweight, a central cause (pituitary adenoma, Sheehan’s syndrome, pituitary hemorrhage, Rathke’s cleft cyst, empty sella, meningioma, hypophysitis), a thyroid related cause (autoimmune hypothyroidism, primary hypothyroidism, goitre, Graves’ disease, thyroid carcinoma, thyroiditis) and assay error.
These diagnoses have been described after additional follow-up for 40 of these patients (81.6%). In 81.6% of the 49 patients who had a normal TSH in combination with an increased free T4, no explanation for the aberrant values was found, no additional investigation had been done and none of these patients had received thyroid inhibitory medication. Causes that were found in the remaining patients are: medication (amiodarone), a thyroid related cause (Graves’ disease, toxic nodule) and assay error. Additional investigation had been performed for four (44.4%) of these patients. One (11.1%) of them started on propylthiouracil.
In four cases of our study population (one decreased free T4 and three increased free T4) the treating physician sent the patient’s blood to the Erasmus Medical Center Rotterdam to check for an assay error. In all cases an assay error was ‘diagnosed’. The treating physician did not record his considerations in any of these cases. See figure 1 for an overall summary.
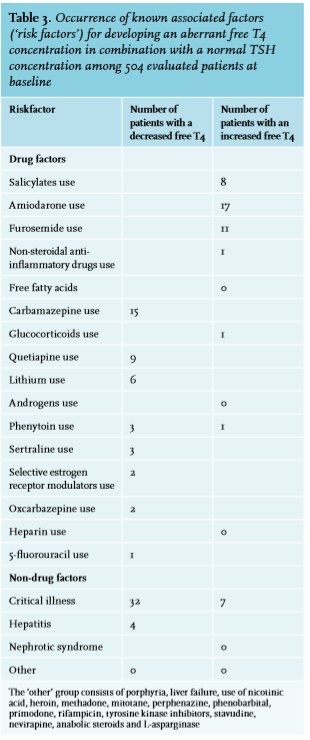
Next to checking for how many patients the treating physician found a cause for the aberrant values, we also checked the medical files for any identifiable cause of aberrant combinations between free T4 and TSH concentrations. In other words: we looked for ‘risk factors’ a physician can identify by performing an interview and physical examination, and by assessing the medical history and medication usage of the patient, so before any additional investigation has been performed. For 123 of the patients with a persistant aberrant free T4 (30.9%) one or more causal factors for aberrant combinations were identified (table 3).
During data collection we also checked for free T3, total T3 and total T4. Total T3 was measured only in 10 patients (2.0%), free T3 and total T4 were not measured. Anti-TPO, anti-Tg and anti-TSH-R did not contribute to further diagnostic workup.
DISCUSSION
In our study, screening for thyroid function yielded a combination of a normal TSH and an aberrant free T4 in 3.3% of the patients.
In the current literature various causes of hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH are discussed, as shown in table 1.
The most common cause is drug related.7-10 For example, anticonvulsants (phenytoin, carbamazepine and phenobarbital) and also rifampicin can increase the metabolic clearance of T4 by enzyme induction.11-12 In addition, it has been demonstrated that amiodarone can inhibit the transport through the plasma membrane which can lead to an elevated free T4 in combination with a normal TSH. Other drugs can decrease the binding of T4 to the thyroxine binding globulin (TBG): salicylates, salsalate and certain non-steroidal anti-inflammatory drugs.7-10
It should be stressed that the effect of a drug on protein binding depends on the dilution factor of a sample in a specific assay. An assay with high dilution is less affected by this drug effect.13 Assay interference may also cause aberrant results.14 A typical example of assay interference is the inhibitory effect of furosemide on free T4 binding to TBG. In a blood tube this effect continues and this may lead to misleadingly high free T4 concentrations. However, in an assay with a high dilution factor this effect is minimalised (see references 9 and 15 for further reading). In the case of unexpected laboratory results the clinician should always be aware of assay errors and ask the clinical laboratory for further research into this matter.
Another reason why free T4 may be aberrant is critical illness. In cases of critical illness, circulating substances, such as a high serum free fatty acid concentration, can prevent T4 binding to the binding proteins. Also deiodination of thyroid hormones can be affected. This may result in either high or low serum free T4 concentrations.16 Of the patients included in our study, 9.8% turned out to be critically ill.
A rare but important reason why the TSH may be normal in combination with a decreased free T4 is central (secondary) hypothyroidism.4,17 Since, among other things, this condition can be related to a pituitary adenoma or external compression on the pituitary gland, and might have serious clinical consequences if missed, central hypothyroidism always needs to be considered. We found a central cause in 3.8% of our population. Other possible causes of hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH include abnormal protein binding of TBG, transthyretin and albumin. In familial dysalbuminemic hyperthroxinemia, for example, binding of T4 to dysalbumin, a structural variant of albumin, is increased. In vivo, this will lead to a high concentration of total T4 and normal free T4 levels. In certain assays, however, this dysalbumin leads to interference and artificially high free T4 concentrations.18
Certain factors may change binding protein concentrations, and thus may increase or decrease the serum concentrations of T4 and T3. Examples are estrogens, hepatitis and drugs like 5-fluorouracil. We did not find these in our population. Also acute psychosis19-20 and reduced thyroxine deiodination can cause hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH.21-24
Finally, one should realize that both intra- and interindividual differences in the hypothalamic-pituitary-thyroid axis setpoint are potential causes of abberant free T4 concentrations.25
This study demonstrates that 3.3% of the patients have a combination of a normal TSH with an aberrant free T4 on testing for thyroid function. 87.7% of the included patients had a decreased free T4 in combination with a normal TSH, while an increased free T4 in combination with a normal TSH was less common (12.3%).
In most medical files we could not ascertain that additional investigation had been done to find an explanation for the aberrancies. Most of the time we could also not find if the physician recognised this aberrancy: in 81.9% of cases no explanation was found for the aberrancies, and also no additional investigation had been carried out. However, after checking the available medical files we could identify a causal factor in 30.9% of the patients with a persistant aberrant free T4.
Potential explanations for the lack of diagnostic workup in a large proportion of cases included in this study could be unawareness of hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH and its causes, as well as the lack of guidelines regarding its management and the assumption that these conditions most often do not have clinical consequences. This assumption may well be incorrect since recent studies showed that free T4 but not TSH is associated with sudden cardiac death26 and depression.27
Recommendations for patients with a normal TSH in combination with an aberrant free T4
Becasue in 21% of the cases in this study aberrancies were not persistent after the test was repeated, we advise physicians who have patients with this condition to remeasure serum free T4 and TSH after two to three months.28 In a recent trial a high number of reverted subclinical hypothyroidism was seen in two out of three patients without any therapy upon remeasurement after three months to three years.29 The time frame of remeasurement in our study was two months to five years. Any easily identifiable causal factor, such as certain medication, should be checked (tables 1 and 3), and non-drug related factors such as critical illness, hepatitis and nephrotic syndrome should be evaluated as well.
When hyperthyroxinemia or hypothyroxinemia in combination with a normal TSH is found, the clinical challenge is to recognize a central cause like pituitary adenoma or external compression of the pituitary gland or hypothalamus. Delay of the diagnosis may have serious medical consequences.
One strategy to follow could be that if free T4 persists to be aberrant after repeated measurement in a non-pregnant patient and without any clear explanation (see table 1 and 3), one should first consult the laboratory to rule out assay interference. If no assay interference can be established, a central (secondary) cause should be considered. Especially when clinical features suggest thyroid dysregulation, the next step would be either imaging (MRI) of the pituitary gland and hypothalamus or pituitary function tests.
Finally, if the aberrancy persists, rare disorders such as thyroid hormone resistance might be considered. This diagnosis may involve identifying a mutation of the thyroid receptor. Figure 2 shows a flowchart with our suggestions for analysis of hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH.
Limitations
This study has several limitations. Incomplete, missing and unreliable information in the medical record may have caused incorrect inclusion or exclusion. This may have caused an incorrect number of explanations given for an aberrant free T4. There is a possibility that the physician did have an explanation for the aberrant free T4, but did not write it down. We only included patients in whom a normal TSH in combination with an aberrant free T4 had been found. In many patients only TSH had been determined and – if normal – no free T4 had been measured. Therefore, the actual number of aberrancies between TSH and free T4 might be much higher.
Since drug-induced interference in thyroid function tests is uncommon in assays with a high dilution factor, this fact can be used to identify or rule out true interference. The assay we used in our study had a high dilution factor. Therefore, the true number of drug-induced abnormal tests is probably lower than reported.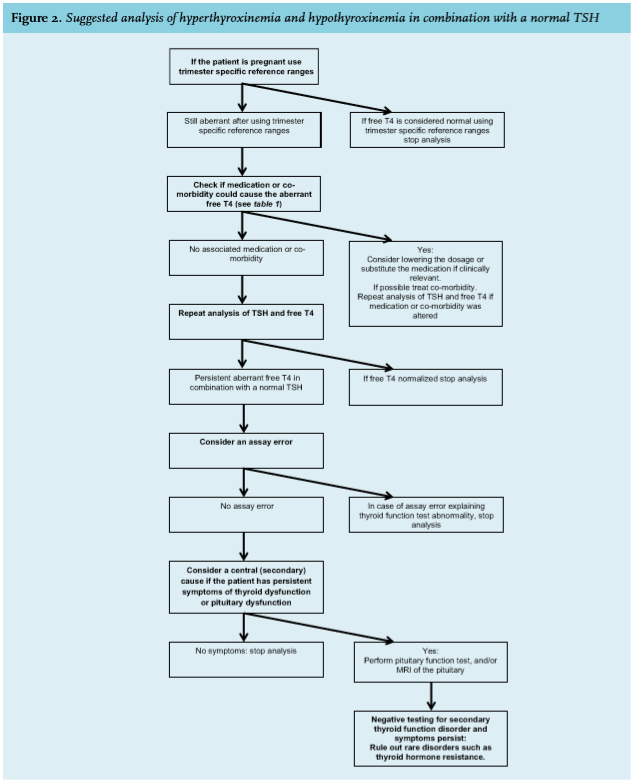
CONCLUSION
This study demonstrates that in our population of patients screened for thyroid dysfunction in a non-university general hospital 334 per 10,000 patients had a normal TSH in combination with an aberrant free T4. We also found that many physicians do not follow-up on this condition or record a causative factor. When medical files are searched thoroughly however, identification of a possible causative factor increases from 14.6% to 30.9%. Therefore, clinicians should be encouraged to check for additional causes of these aberrant free T4 entities. The largest challenge is not to miss serious underlying conditions like secundary hypothyroidism. We present a possible strategy for analyse hyperthyroxinemia and hypothyroxinemia in combination with a normal TSH. We believe it is important to deploy a similar strategy in guidelines about thyroid disorders. Future studies on this topic should be performed to gain more insight about the best way to follow-up on this condition.
ACKNOWLEDGMENTS
We thank the staff of the clinical laboratory of Alrijne Hospital for their help with data collection.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES