KEYWORDS
Osteoporosis, type 2 diabetes mellitus (T2DM), hip fracture, diabetes complications severity index (DCSI)
INTRODUCTION
Osteoporosis is a bone condition defined by low bone mass, decreased bone quality or increased fragility, and increased fracture risk.1,2 It is a major public health problem because of its associated fractures and the resulting complications, including mortality. Therefore, identifying populations at risk of osteoporosis and fracture is critical for the prevention of the disease and further intervention. Many risk factors for osteoporosis have been identified, such as age, being post-menopausal, currently smoking, and excessive intake of alcohol, which were incorporated into the Fracture Risk Assessment Tool (FRAX) developed by the World Health Organisation. Nevertheless, diabetes may be an overlooked a risk factor despite substantial evidence indicating that type 2 diabetes mellitus (T2DM) is associated with a higher risk of hip fracture, independent of sex, increased body mass index, or other classical risk factors of osteoporosis.3-6 In addition, while bone mineral density plays a major role in the current risk assessment tool, current evidence reveals a discrepancy in fracture risk and bone mineral density in patients with T2DM.7 Most studies have shown increased bone mineral density in T2DM patients;8,9 however, the risk of fracture is still higher compared with that of non-diabetic patients.
FRAX, as the most widely used risk assessment tool for osteoporosis, may therefore underestimate the risk of fracture in diabetic patients.10,11
Considering underestimation of fracture risk in diabetic osteoporotic patients, we highlight the correlation between T2DM and osteoporotic fractures. Furthermore, while the relation between T2DM and osteoporosis has been widely examined in previous studies, no study has addressed whether the severity of T2DM affects the risk of fracture in patients with osteoporosis. To identify the population at risk of hip fracture, we conducted a retrospective study of osteoporotic patients aged over 40 years in a regional hospital in central Taiwan. In this study, we try to identify possible risk factors for hip fracture, and examine the correlation between the severity of T2DM and risk of hip fracture in patients with osteoporosis.
MATERIALS AND METHODS
Study design and subjects
This was a retrospective study. The data were obtained from the database of Puli Christian Hospital, a regional hospital in central Taiwan. The database contains information such as patient profiles (date of birth, sex, ethnicity), inpatient and outpatient records, laboratory data, examination results, and all previous diagnoses classified according to the International Classification of Diseases, Ninth Revision (ICD-9). The data, such as patient profiles, inpatient and outpatient diagnoses, and records of prescription use, are sent to the Bureau of National Health Insurance (NHI) for reimbursement purposes, and further incorporated into the research database of the NHI, which has often been used in high-quality epidemiological research in Taiwan.
By using the ICD-9 codes, we identified patients who received a diagnosis of osteoporosis between 2006 and 2010. Participants were selected based on the following criteria: 1) age greater than 40 years, 2) diagnosis of osteoporosis (ICD-9 code 733.0) in 2006-2010, and 3) at least three visits to the outpatient department or one admission12 between 2006 and 2015. Samples were excluded because of 1) death not related to hip fracture during the follow-up period of 2006-2015, 2) insufficient follow-up, 3) referrals from other hospitals, and 4) hip fracture before the diagnosis of osteoporosis or T2DM. Information including the duration of diabetes, HbA1c (measured on the diagnosis of T2DM), and previous medical history was obtained by reviewing patients’ medical records. Any event of hip fracture occurring between 2006 and 2015 was considered in the outcome of this research.
Evaluation of diabetes severity: Diabetes Complications Severity Index
The severity of the diabetes of all the patients was graded according to the Diabetes Complication Severity Index (DCSI). The DCSI was developed by Young et al.13 in 2008 and it comprises seven categories of diabetes complications: cardiovascular disease, nephropathy, peripheral vascular disease, cerebrovascular events, neuropathy, retinopathy, and metabolic complications. The DCSI was developed to model the severity of diabetes complications at any point in time. Except for neuropathy, which is categorised into only two levels (0 and 1), all other complications can be graded in three levels (0, 1, and 2) based on the severity. Therefore, a total score of 13 is possible for the DCSI, with a minimum of 0. In our study, all patients with T2DM were stratified according to the DCSI to highlight the correlation between the severity of diabetes and the risk of hip fracture in osteoporotic patients.
Statistical analysis
The t-test and chi-square test were used to compare the baseline characteristics between 1) the hip fracture group and the non-fracture group, and 2) groups of patients with T2DM stratified according to the DCSI. A logistic regression model was used to examine the relationship between the severity of diabetes complications and the risk of hip fracture in the osteoporotic patients. Odds ratios (ORs) were calculated through both univariate analysis and multivariate logistic regression; in the multivariate analysis, other possible confounding variables were adjusted for.
Osteoporotic patients with T2DM were stratified according to the DCSI. Stepwise model selection for the series of model comparisons was used to identify the most effective predictive markers for the risk of fracture in patients with osteoporosis. In addition, c-statistics (area under the curve, AUC) were introduced to determine whether grouped stratification of the DCSI (i.e., DCSI 0-1, DCSI 2-3, DCSI > 3) was more effective in predicting fracture than linearisation or simple count categorisation of the DCSI. By using this method, we intended to determine a cut-off point of the DCSI for intervention purposes in patients with osteoporosis.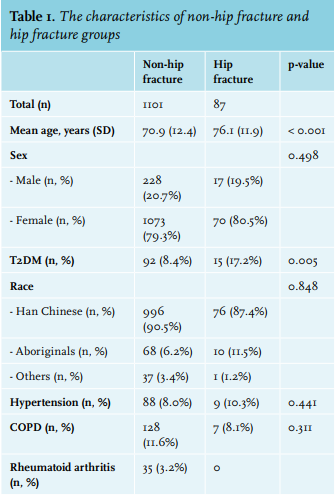
RESULTS
A total of 1244 patients were recruited by reviewing the patients’ medical records between 2006 and 2010. Among the 1244 patients, 56 were excluded for the following reasons: death not related to hip fracture (24), insufficient follow-up (27), and referrals from other hospitals (5). A total of 1188 patients were considered eligible for final analysis. Of these 1188 patients, 87 had hip fractures during the follow-up period.
Comparing the baseline characteristics between the hip fracture group and the non-fracture group (table 1) revealed that the patients who had fractures were significantly older, with a mean age of 76.1 years in comparison with 70.9 years (p < 0.001). Among those with hip fractures, the prevalence of T2DM was significantly higher at 17.2% compared with 8.4% (p = 0.005). Other variables including sex, ethnicity (Han Chinese, aboriginal, others), presence of COPD, hypertension, and rheumatoid arthritis were not associated with a significant difference in the prevalence between the two groups. This observation suggests that T2DM is a risk factor for hip fracture in patients with osteoporosis.
Among all patients with osteoporosis, 107 previously received a diagnosis of T2DM. Of the patients with T2DM, 43 (40.2%) had a DCSI of 0-1, 35 (32.7%) had a DCSI of 2-3, and 29 (27.1%) had a DCSI > 3 (table 2). One-way ANOVA for comparing the baseline characteristics revealed a significant difference in the mean duration of diabetes between the groups. Post hoc tests showed a significant difference between the DCSI 0-1 group and the DCSI > 3 group (p < 0.05). The patients with a higher DCSI tended to be older and have a higher HbA1c level on diagnosis of T2DM.
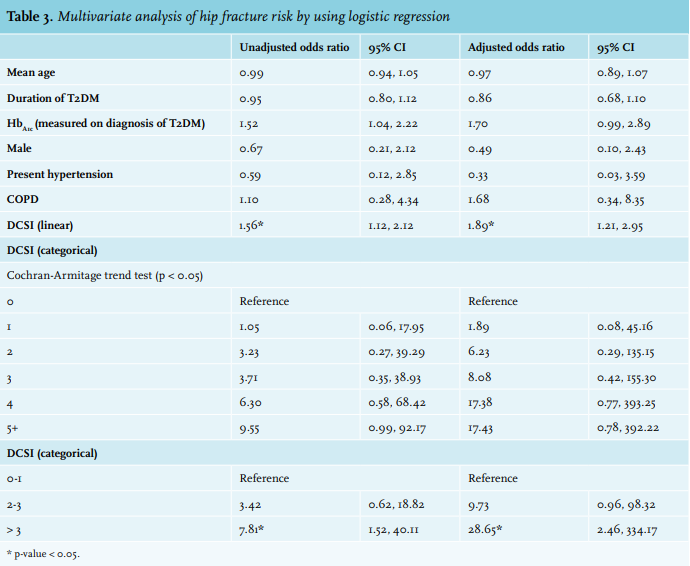
Of the 107 diabetic osteoporotic patients, 15 suffered hip fractures. The adjusted OR of hip fracture is shown in table 3. Both univariate and multivariate analyses using logistic regression were performed. When the DCSI was considered a linear variable, the OR was 1.56 (95% confidence interval [CI] = 1.12-2.12) in univariate analysis, and it was 1.89 (95% CI = 1.21-2.95) in multivariate analysis after adjustment for age, duration of diabetes, HbA1c on diagnosis of T2DM, presence of COPD, and hypertension. When the linear form of the DCSI was replaced with the categorical DCSI, a significant trend of increasing risk in patients with higher diabetes complication severity was noted (Cochran-Armitage trend test, p < 0.05). When the patients were divided into three categories according to the DCSI severity, the DCSI > 3 group had a significantly higher risk compared with the DCSI 0-1 group (OR = 7.81, 95% CI = 1.52-40.11 in univariate analysis; adjusted OR =28.65, 95% CI = 2.46-334.17 in multivariate analysis).
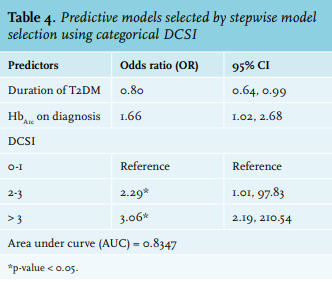
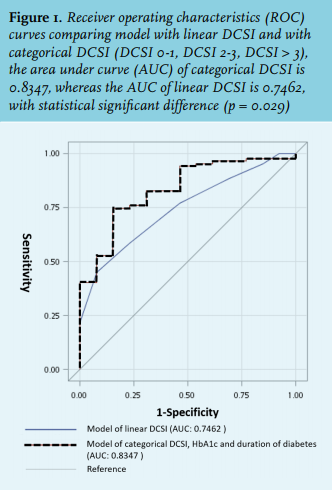
By using stepwise model selection, models were established for a categorical variable (DCSI 0-1, DCSI 2-3, and DCSI > 3) and a linear variable of the DCSI. The model with the categorical DCSI contained two other variables, the duration of diabetes and HbA1c level on diagnosis (table 4); in the other model, the linear DCSI was the only variable that was associated with a significant difference in fracture risk. For model comparison, we established receiver operating characteristic (ROC) curves of both models: the AUC was 0.7462 for the model with the linear DCSI, and the AUC was 0.8346 for the model with the categorical DCSI, with the difference being significant (p = 0.029) (figure 1). This result suggests that the model containing the categorical DCSI is slightly more effective in predicting hip fracture risk in patients with osteoporosis with T2DM.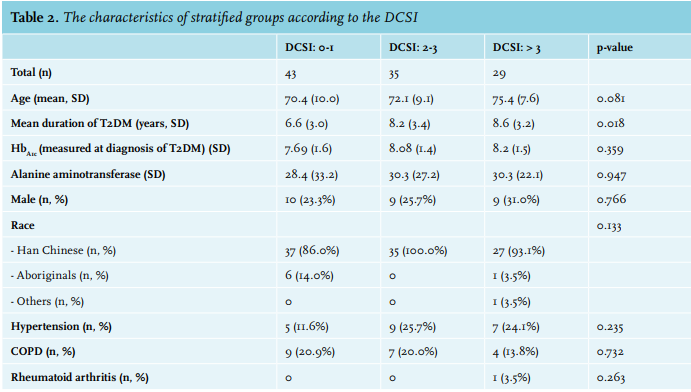
DISCUSSION
This was the first retrospective study to determine whether diabetes severity is associated with the risk of hip fracture in osteoporotic patients. The results of this study not only confirm that T2DM is a risk factor for hip fracture but also indicate that patients with greater diabetes severity are at a higher risk of hip fracture. In addition, in the predictive model selected for our study, three predictors associated with hip fracture in osteoporotic patients were identified: the severity of diabetes, HbA1c level on diagnosis of T2DM, and the duration of diabetes.
T2DM in osteoporosis
Several mechanisms have been proposed to explain the relationship between diabetes or hyperglycaemia and osteoporosis. T2DM is associated with increased bone mineral density8-9,14 and an increased risk of fracture.7,15 The early studies attributed the increased fracture risk to the use of thiazolidinedione16 or insulin17 and the increased frequency of falling to diabetes complications.18 A study reported that diabetes complications, such as autonomic neuropathy, peripheral neuropathy, retinopathy, and syncope related to hypoglycaemia, are associated with an increased frequency of falling.19 However, when the frequency of falling is controlled for, T2DM still remains an independent risk factor for fracture.3,20 Additionally, the observation periods of many studies included the time period prior to the widespread use of thiazolidinedione;21 thus, the use of thiazolidinedione may not fully account for the increased risk of fracture in T2DM patients. Recently studies have suggested that some bone properties (e.g., alterations in the trabecular compartment of bone,22 micro-architectural deficits,23 accumulation of advanced glycation end products24,25) that are undetectable through bone densitometry also contribute to the risk of fracture in diabetic patients.
Although the mechanism of the increased risk of fracture in T2DM is not yet fully understood, it should be noted that T2DM has implications for bone strength in multiple aspects. In addition to fall frequency, skeletal resorption and mineralisation defects are associated with hyperparathyroidism related to renal dysfunction, a common complication of T2DM.26 The microvascular disease related to T2DM may interfere with blood flow to the bone marrow, thus affecting the microenvironment and local remodelling of the bone.27,28 While the DCSI provides a general impression of diabetes severity and has been validated in predicting adverse outcomes of T2DM,13,29 it may also be valuable in assessing bone complications. Our study established that a higher severity of diabetes is associated with an increased risk of hip fracture. This information may assist in early identification of a high-risk group of osteoporotic patients with T2DM.
Duration of T2DM and the role of HbA1c in risk assessment
In the predictive model selected, when the HbA1c level and a high DCSI were considered risk factors, the duration of diabetes served as a mildly protective factor in the diabetic osteoporotic patients. We reviewed the duration of diabetes in those who suffered hip fractures, and the data showed a mean duration of 5.7 years in the DCSI 0-1 group, 8.01 years in the DCSI 2-3 group, and 7.0 years in the DCSI > 3 group. The HbA1c measured on diagnosis was 7.8 in the DCSI 0-1 group, 8.8 in the DCSI 2-3 group, and 9.0 in the DCSI > 3 group. The data revealed that, in our study, osteoporotic patients with diabetes who are at risk of hip fracture tend to have a shorter diabetes duration, a higher HbA1c level on diagnosis, and higher diabetes severity. A possible explanation is that the patients recruited in our study who later developed hip fracture did not receive a diagnosis at the onset of diabetes and generally presented with a higher HbA1c on diagnosis. Since our hospital is located in the mountainous area of central Taiwan, where many aboriginal tribes reside, medical accessibility may not be similar to urban areas due to inconvenience of transportation.30
According to the American Diabetes Association, undiagnosed diabetes is not uncommon, with as many as 27.8% of diabetic patients not receiving a diagnosis.31 Since it may be difficult to determine the actual onset of diabetes, HbA1c screening may therefore have value not only in diagnosing diabetes but also as a predictive marker for complications. A previous study reported that the pre-intervention HbA1c is significantly associated with the risk of complications such as diabetic retinopathy, and is associated with an increased risk of fracture.32 In addition, a study confirmed that long-standing glycaemic exposure (with a threshold of the mean HbA1c ≥ 6.5) increases the risks of vascular complications and death,33 which also suggests that HbA1c is valuable in predicting the risk of future complications.
In our study, instead of using the mean HbA1c in the analysis, we employed the HbA1c value on diagnosis of T2DM. This is because the increasing awareness of ‘metabolic memory’ has suggested that diabetic stresses persist despite glucose normalisation.34 Based on the theories, recent studies have indicated that intensive glucose control offers no protection against cardiovascular risk and mortality in T2DM.35,36 A study reported that the prevalence of osteoporosis and frequency of fractures were higher in long-standing T2DM, irrespective of blood glucose control.37 While bone tissue may be one of the memory’s target organs, the mean HbA1c may be of less value in risk assessment compared with the HbA1c level on the onset of the disease. In our study, we established that the HbA1c level on diagnosis of T2DM is associated with a greater risk of hip fracture and therefore may be useful for predicting bone complications.
To conclude, patients who later had hip fractures during follow-up generally presented with a higher HbA1c level on diagnosis of T2DM and a higher severity of disease, which may serve as surrogate predictors in addition to the current screening tools for early prediction in osteoporotic patients, particularly because FRAX may underestimate the risk of fracture in diabetic patients.7,8
Limitations
This was a retrospective study with ICD-9 coding from the database, and it has several limitations. First, the patients were enrolled based on the clinical diagnosis of osteoporosis during the follow-up period, and the severity of osteoporosis or the extent of hip fracture could not be assessed. Second, the diagnosis of osteoporosis and diabetes was made by different physicians with different methods or criteria. However, the National Health Insurance program of Taiwan was implemented in 1995, and most Taiwanese were covered by this insurance. All insurance claims should be scrutinised by medical reimbursement specialists. Although osteoporosis was diagnosed by individual physicians who may define the condition using different methods, such as dual-energy X-ray absorptiometry or quantitative ultrasound, the diagnoses in this study were highly reliable. Similarly, the diagnosis of diabetes was made by either HbA1c or fasting glucose, depending on the specialist. Third, although we could review certain baseline characteristics of the participants in our study, information regarding patients’ lifestyles (e.g., amount of alcohol intake and smoking) is lacking in the database. Finally, we used the DCSI to evaluate the severity of T2DM; the DCSI is an unweighted index which does not independently test adverse outcomes associated with each complication.11
Although this study has several limitations, it realistically reflects the relationship between the severity of T2DM and risk of hip fracture in osteoporotic patients.
CONCLUSION
The severity of T2DM is associated with an increased risk of hip fracture in osteoporotic patients. The categorical DCSI (DCSI > 3), HbA1c level on diagnosis of T2DM and duration of diabetes facilitate predicting the risk of hip fracture. Physicians should pay attention to osteoporotic patients presenting with a high HbA1c level on diagnosis of T2DM and a higher DCSI because of their vulnerability to hip fracture.
DISCLOSURES
The authors declare no conflict of interest.
REFERENCES