KEYWORDS
Temozolomide, pituitary carcinoma, prolactinoma
INTRODUCTION
About 15% of all new primary tumours of the brain and central nervous system consist of pituitary adenomas.1 Pituitary adenomas are classified according to their pattern of hormonal secretion, with prolactinomas and non-functioning pituitary adenomas as the most common subtypes.2 Pituitary carcinomas form an extremely rare, aggressive variant of pituitary adenomas which – by definition – involve cerebrospinal and/or systemic metastases and account for 0.1% of the pituitary tumours.1 These tumours have an average survival of less than four years because of a rapid and invasive growth pattern, and relapse frequently despite the current therapies.3 Some pituitary tumors exhibit clinically aggressive behavior that is characterized by tumor recurrence and continued progression despite repeated treatments with conventional surgical, radiation and medical therapies. Temozolomide, an alkylating oral chemotherapeutic agent, is widely used to treat glioblastoma.4,5 We present a case of pituitary carcinoma with a dramatic and durable complete response to temozolomide.
CASE REPORT
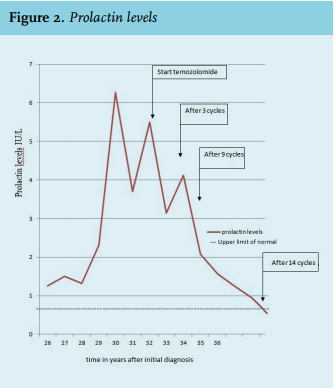
A 37-year-old man underwent a craniotomy with subtotal resection of a pituitary tumour, which was discovered during evaluation for chronic headaches. Histological examination revealed a prolactinoma and adjuvant radiotherapy, with a total dose of 50 Gy, and suppletion hormonal therapy were administered. Over the next 21 years, follow-up consisted of repeated measurement of the prolactin level and showed stable disease. After those 21 years, elevated prolactin and growth hormone levels (earliest recorded levels: prolactin level 13.50 IU/l (reference values 0.10-0.65) and IGF-1 342 ng/ml (reference values 52-162)) led to MRI scanning showing progression of the residual lesion in the sellar region, suggesting mixed prolactinoma and growth hormone secreting tumour. Therefore the patient was treated with bromocriptine, an oral dopamine D2 receptor antagonist. Because of intolerance, the patient was switched to cabergoline, a long-acting dopamine agonist specific for the D2 receptor, and successfully treated for one year (until 22 years post-surgery). Aged 60 years, 23 years after the initial diagnosis, he underwent surgery for a meningeal tumour at the right jugular foramen which was found on a routine follow-up MRI scan. Histology revealed pituitary adenoma. Since the resection was irradical, the patient underwent local postoperative radiotherapy with a total dose of 50.4 Gy (no images available); after this treatment no neurological problems where observed. Twenty-three years after the initial surgery, a transsphenoidal resection of the residual lesion was performed as the prolactin and IGF-1 levels increased and the tumour proved resistant to cabergoline. Thirty years after the first operation further progression was observed with increasing prolactin concentrations up to 6.3 IU/l, normal IGF-1 and an increased pituitary lesion on MRI; he received stereotactic radiotherapy with a total dose of 50.4 Gy as 30 years had lapsed between the first and the current, third, radiation therapy, while the planned radiation field of the current treatment did not overlap with the field of the second treatment. Two years later after stereotactic radiotherapy (32 year since first presentation) the patient experienced memory problems, gait instability and lower back pain irradiating to the legs. On neurological examination, minor sensorimotor abnormalities of both legs were found consistent with painful lumbosacral polyradiculitis. Prolactin levels remained increased at 3.14 IU/l and MRI showed multiple gadolinium-enhancing nodular lesions in the lumbar spine as well as two at the cervical level, consistent with drop metastases of the prolactinoma (figure 1) with stable disease in the brain. Cerebrospinal fluid (CSF) analysis revealed mild lymphocytic pleiocytosis (leucocytes 12 x 106/l; 79% lymphocytes) with an increased protein level of 1.66 g/l; cytological examination was negative for tumour cells. The diagnosis of pituitary carcinoma with leptomeningeal metastases was made based on rapidly progressive symptomatology (motor impairment with increasing fall risk), medical history, radiology and CSF abnormalities, despite the negative CSF cytology. On the advice of the multidisciplinary tumour board, temozolomide chemotherapy 200 mg/m2 /day days 1-5 every 4 weeks (total dose of 500 mg per day) was started in the absence of feasible local treatment options. After 4 cycles, the patient experienced improvement of his gait. Biochemical and radiological evaluation after 9 cycles revealed partial remission. After 14 cycles normalisation of prolactin levels was reached and maintained since then (figure 2). As the treatment was well tolerated, the patient continued therapy for 21 cycles without dose reductions. Thirty-four years after first presentation, it was decided to discontinue chemotherapy as clinical, biochemical and radiological complete remission was obtained. The most recent neurological, biochemical and radiological evaluation, 34 months after completion of temozolomide, showed continued complete remission.
On retrospective tissue review, MLPA analysis of metastasis tissue showed no hypermethylation of O(6)-methylguanine-DNA methyltransferase (MGMT) and normal MLH1, MSH2, MSH6 and PMS2 gene profiling. The fraction of proliferation determent with monoclonal antibody Mib-1, which is comparable with Ki67,2 was only 5%. 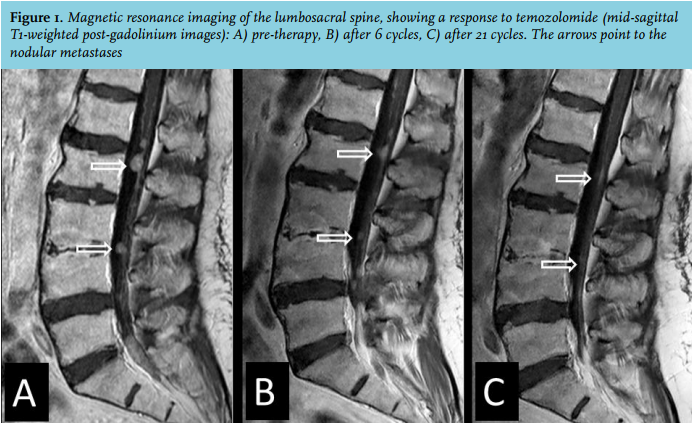
DISCUSSION
In the World Health Organisation (WHO) classification for pituitary tumours of 2004, the term ‘pituitary carcinoma’ is restricted to tumours with proven cerebrospinal and/or systemic metastases. Aggressive pituitary adenoma is used for medical and radiotherapy resistant pituitary lesions. Distinction between pituitary adenoma and carcinoma based on morphology remains challenging. Increased (> 3%) Ki-67 labelling index and p53 immunoreactivity suggest aggressive potential of the tumour or malignant transformation.2 Nowadays treatment consists of resection, radiotherapy in unresectable or recurrent cases, and dopamine antagonists for prolactinomas. No registered treatment is available for patients in whom these treatments fail. This is most strikingly the case for pituitary carcinomas, since the dissemination in the central nervous system is rarely amenable to resection and craniospinal radiotherapy is associated with considerable toxicity. We found 25 articles1,3,6-28 in the literature on pituitary carcinomas (n = 79) or treatment-resistant pituitary adenomas that were treated with temozolomide since the first publication in 2006. Clinical efficacy (partial or complete response or stable disease) was observed in 39 cases; a recent review estimated response rates to be 58% in aggressive pituitary adenomas and 55% in pituitary carcinomas.28 The overall experienced toxicity was mild.
pituitary carcinomas (n = 79) or treatment-resistant pituitary adenomas that were treated with temozolomide since the first publication in 2006. Clinical efficacy (partial or complete response or stable disease) was observed in 39 cases; a recent review estimated response rates to be 58% in aggressive pituitary adenomas and 55% in pituitary carcinomas.28 The overall experienced toxicity was mild.
Given the rarity of the diagnosis of pituitary carcinoma, it is unlikely that randomised studies will be performed. The current case with local radiotherapy and dopamine agonist resistant prolactin producing pituitary carcinoma adds to the available literature by underscoring the potential efficacy of temozolomide and good tolerability, even in the setting of biochemically active, symptomatic and widespread leptomeningeal metastases.
Temozolomide has proven efficacy in the treatment of glioblastoma. In these malignant primary brain tumours, hypermethylation of the promoter of MGMT, a gene involved in DNA repair, is predictive of efficacy of temozolomide. MGMT hypermethylation has been found in some pituitary adenomas.5 In our case, MGMT was not hypermethylated. Although this may be due to imperfections in the currently available MGMT assays, this finding suggests that efficacy of temozolomide cannot be predicted solely on the basis of MGMT status.
CONCLUSION
In this case of pituitary carcinoma with extensive leptomeningeal spread, associated debilitating neurological symptoms, and proven resistance to registered therapies, prolonged treatment with temozolomide led to a complete and durable remission and clinical improvement. These observations lend further support to the role of temozolomide in refractory pituitary tumours.
DISCLOSURES
No grant support needs to be reported. Conflict of interests: none declared.
REFERENCES