KEYWORDS
Neuroimaging, intracerebral haemorrhage, clinical neurology, MRI, toxicology, stroke
INTRODUCTION
The ethnicity of a patient and cultural factors are rarely the key to the diagnosis in acute neurology. While certain metabolic disorders are associated with ethnic groups, rare neurodegenerative disorders are linked to relatively isolated communities, and multiple sclerosis is associated with geographic latitude, the cultural background of a patient is seldom helpful in neurological emergencies. Haemochromatosis, cystic fibrosis, coeliac disease, and multiple sclerosis are relatively common in Ireland, and many of these conditions have a strikingly low incidence in East-Africa and in the Middle-East. Thalassaemia, Bechet’s disease, and sickle-cell anaemia on the other hand have a low incidence on the island of Ireland. Routine screening in Irish emergency departments reflects the commonest presentations and toxicology tests typically include amphetamines, opiates, paracetamol, benzodiazepines, tricyclic antidepressants, cannabis, and alcohol. Serum and urine toxicology tests are routinely performed in first seizures, unexplained behavioural disturbances, patients with previous self-harm and in other vulnerable patient cohorts. While neurologists worldwide take pride in the fast integration of subtle clinical findings and radiological cues, cultural factors are often overlooked. We present the case of a critically ill young man from Somalia whose radiological presentation was initially a conundrum.
CASE REPORT
A 45-year-old right-handed Somalian man with a background of hypertension and chronic kidney disease, was brought to the hospital with agitation, confusion and severe headaches. His Glasgow Coma Scale score was initially 15/15 and his blood pressure was 220/130 mmHg. Shortly after arrival, he developed a left hemiparesis, then a cluster of seizures. He was intubated and computed tomography of the brain revealed a large right temporo-parietal intraparenchymal haematoma with intraventricular extension, a small left parietal haematoma, and hydrocephalus. Four-vessel digital subtraction angiography did not identify aneurysms or arteriovenous malformations, but was suggestive of focal pericallosal artery constriction, without definite evidence of vasoconstriction or beading of any other arteries. A left external ventricular drain was inserted and the neurology service was consulted. The patient was first assessed while ventilated and on propofol sedation. His blood pressure remained 190/100 mmHg despite aggressive antihypertensive therapy, his fundoscopy showed evidence of grade III hypertensive retinopathy. He was hyperreflexic in all four limbs and had absent corneal and vestibuloocular reflexes.
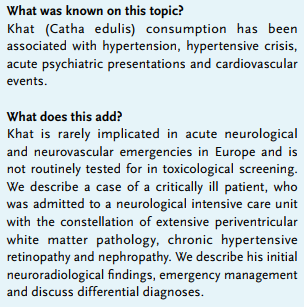
His urgent MRI brain scan revealed confluent pontine, mesencephalic, thalamic and periventricular white matter hyperintensities on FLAIR and T2-weighted brain imaging in addition to the right temporo-parietal haemorrhage (figure 1). Based on the MRI findings, the differential diagnosis included hypertensive encephalopathy, posterior reversible encephalopathy syndrome (PRES), acute toxic leukoencephalopathy, vasculitis and infective aetiologies, including fungal and flavivirus infections.
The patient’s renal profile revealed a creatinine of 393 μmol/l and urea of 23.3 mmol/l. The 24-hour urinary catecholamine and metanephrine levels were normal and blood film and haematological screens showed no evidence of thrombocytopenic purpura, haemolyticuraemic syndrome, disseminated intravascular coagulation or microangiopathic haemolytic anaemia. While serum and urine toxicology were negative for amphetamines and cocaine metabolites, the constellation of chronic hypertensive end-organ damage and the acute hypertensive crisis led to the suspicion that the patient may have consumed Khat. 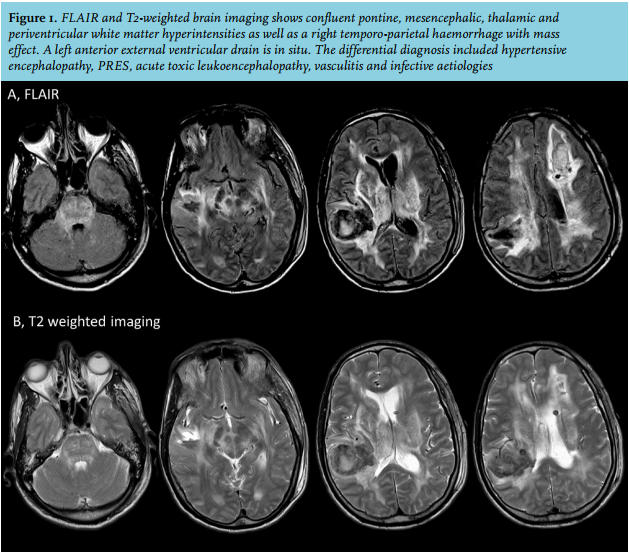
DISCUSSION
The leaves of the Khat plant (Catha edulis) contain cathinone, an amphetamine-like alkaloid. Chewing of Khat is uncommon in Ireland, but has a long tradition in Yemen, Ethiopia, Sudan and Somalia. It has been widely used since the 7th century and its cultivation in the region predates coffee production.1 It has been associated with chronic hypertension,2 acute hypertensive crisis,3 psychiatric,4-6 cardiac1,7 and cerebrovascular events.8,9 Our suspicion was corroborated by family members and neighbours who confirmed that the patient had been consuming copious amounts of Khat prior to his admission.
While our patient has survived the acute phase, he acquired considerable long-term deficits. Despite intensive multidisciplinary neurorehabilitation efforts, he has only made limited functional gains. Sadly, he remains essentially non-verbal and unable to mobilise independently. From a radiological perspective, the acute haemorrhages showed gradual resolution, but gliotic changes ensued. The extensive periventricular white matter changes showed only partial improvement.
The case showcases a relatively rare cause of toxic leukoencephalopathy. In our view, it also highlights how cultural factors and meticulous history taking may be the key to explaining seemingly disparate clinical cues.
DISCLOSURES
Dr Bede is supported by the Health Research Board (HRB-Ireland; HRB EIA-2017-019), the Irish Institute of Clinical Neuroscience IICN – Novartis Ireland Research Grant, and the Iris O’Brien Foundation. The other authors have no disclosures to report.
REFERENCES