Increased blood glucose variability has been associated with higher mortality in critically ill patients, and was therefore proposed as a quality measure of glucose control in the intensive care unit (ICU).1-5 However, most studies related to glucose variability have not adjusted for potential confounders of this association, such as the presence of blood glucose control, the frequency with which glucose is measured, and the severity of illness.6
We hypothesised an independent association between the blood glucose level and hospital mortality, even when adjusting for such potential confounders. This study comprises a secondary analysis of an earlier completed implementation project of a glucose control guideline.7 The glucose variability was measured for patients from three mixed medical-surgical ICUs during two periods: one year before and one year after the implementation of the new glucose control guideline. This new guideline aimed at a blood glucose target range of 80 - 110 mg/dl, instead of the glucose level < 150 mg/dl in the before period, and required more frequent glucose measurements.7,8
Patient data were extracted from the National Intensive Care Evaluation (NICE) registry. Readmitted patients, those spending less than 24 hours on the ICU, and patients with less than three glucose measurements were excluded from the present analysis.
For blood glucose variability, we used three common measures: the standard deviation of the glucose levels, the mean absolute glucose, and the mean amplitude of glycaemic excursions (MAGE).1 We selected three widely used measures of the quality of blood glucose control: mean blood glucose level, the frequency of glucose measurements, and the incidence of severe hypoglycaemia (defined as a glucose < 40 mg/dl).
We used univariate and multivariate logistic regression analysis to estimate and test the association between measures of glucose variability and hospital mortality. The multivariate logistic regression analysis for each measure of glucose variability included the variables that were suggested as confounders as they meet the criteria for confounding: severity of illness (expressed as APACHE II score); the overall blood glucose level (expressed as the mean blood glucose of the entire stay of the patient in the ICU); blood glucose measurement frequency (expressed as the mean interval between measurements); having at least one severe hypoglycaemia event (< 40 mg/dl blood glucose level); and the specific ICU.
A total of 2175 patients met the inclusion criteria: 1132 admitted before and 1043 after implementation of a new guideline for glucose control. Standard deviation and mean absolute glucose, but not MAGE, increased significantly after implementation of the new guideline. Results of the univariate/multivariate analysis are shown in table 1. All measures of glucose variability were associated with hospital mortality in the univariate analysis. After adjustment has been made for all covariates including admission type, the period (before/after implementation), APACHE score, measurement interval, mean BGL, severe hypoglycaemia, hospital, and interaction between hospital and mean BGL, the multivariate analysis showed that none of the glucose variability measures were independently associated with hospital mortality. The result did not change when we stratified patients into medical and surgical patients (data not shown).
Our findings stand in contrast to previous studies, which reported on an independent association of measures of glucose variability with mortality.1-5 One possible explanation for the discrepancies is that the other studies did not adjust for all identified confounders. We had the unique opportunity to do that by investigating the behaviour of measures of glucose variability and their association with hospital mortality in a multicentre study before and after the implementation of a new blood glucose control guideline.
Our findings show that comparison among study results on measures of glucose variability is difficult and requires accounting for various confounders including the presence of a blood glucose control regime, severity of illness, overall glucose level and measurement frequency.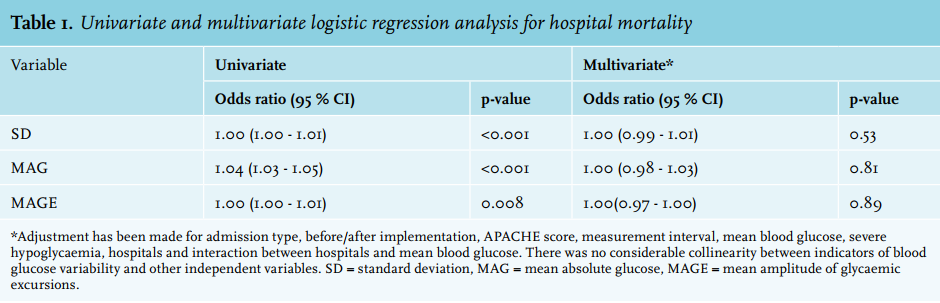
REFERENCES