DIAGNOSIS
Initial ultrasound examination showed pericardial effusion without any signs of cardiac tamponade (figure 3).
Blood cultures and urinary antigen tests suggested infection with Streptococcus pneumoniae. Pericardiocentesis revealed pericardial effusate with leukocyte counts > 10 x 109/l and a lactate dehydrogenase concentration of 3516 U/l. Pneumonia, sepsis with multiple organ failure and purulent pericarditis, all due to Streptococcus pneumonia infection, were diagnosed. Treatment was initially started with amoxicillin and ciprofloxacin and later converted to benzylpenicillin for two weeks when cultures became available. Mechanical ventilation was temporarily required because of respiratory insufficiency and pericardial drainage was performed because of signs of cardiac tamponade and inadequate infectious control. The patient was admitted to the intensive care unit for several days and then gradually recovered during a four-week hospitalisation. Six months later, fibrotic changes of the right lung remained, while the pericardial effusion had resolved completely.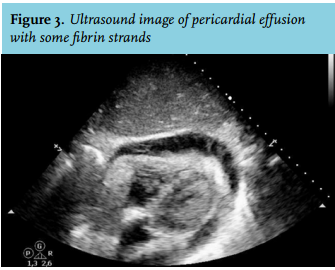
The incidence of infectious purulent pericarditis has clearly decreased after antibiotics became available in the 1940s and is nowadays mainly observed in immunocompromised patients, after cardiothoracic surgery, and/or other predisposing conditions. In the pre-antibiotic era streptococcal pericarditis was relatively common, mostly preceded by pneumonia. In the current antibiotic era, infectious purulent pericarditis is more often caused by Staphylococcus aureus and Gram-negative micro-organisms. Other potentially causative infections are diverse and include tuberculosis and candidiasis.
All patients with purulent pericarditis are reported to demonstrate leucocytosis and tachycardia. Other signs, such as pericardial friction rubbing, pulsus paradoxus, and signs of right-sided heart failure, are not always present. Echocardiography appears to be an important instrument for making clinicians consider the diagnosis of purulent pericarditis.1
When left untreated, purulent pericarditis is uniformly fatal.2,3 Treatment includes systemic antibiotics, pericardiocentesis, and/or surgical pericardial drainage. The last two may be needed in cases of cardiac tamponade and inadequate infectious control with antibiotics alone. Intrapericardial instillation of antibiotics has been evaluated but appeared of no use.3
CONCLUSION
Purulent pericarditis is a rare complication of pneumonia caused by Streptococcus pneumoniae. Because of the high mortality, rapid recognition and treatment are required in order to prevent haemodynamic instability and achieve infectious control.
DISCLOSURES
The authors declare no conflicts of interest.
REFERENCES