KEYWORDS
Glycaemia, intraperitoneal insulin, subcutaneous insulin, type 1 diabetes mellitus, quality of life
INTRODUCTION
Treatment of type 1 diabetes mellitus (T1DM) consists of insulin administration or pancreas (islet cells) transplantation. In most patients, insulin is administered subcutaneously using multiple daily injections (MDI) or continuous subcutaneous insulin infusion (CSII) using an external pump. Although most patients achieve acceptable glycaemic control using subcutaneous (SC) insulin, some patients fail to reach adequate glycaemic control or have frequent hypoglycaemic episodes.1 Continuous intraperitoneal insulin infusion (CIPII) with an implantable pump (figure 1) is a treatment option for such patients.
Of the three randomised clinical studies that compared CIPII with SC insulin treatment in T1DM patients, two reported short-term HbA1c improvements of 8 to 14 mmol/ mol [0.76 to 1.28%] without an increase in hypoglycaemic episodes and one did not find any differences between therapies.2-4 CIPII has also been reported to lead to small improvements in health status, general quality of life (QoL) and treatment satisfaction as compared with SC therapy.5,6 Nevertheless, during the subsequent six years of follow-up among patients treated with CIPII, the short-term improvements in both HbA1c and QoL reported in the randomised studies disappeared and levelled with the values these patients had during intensive SC insulin therapy, while improvements in the number of hypoglycaemic episodes and treatment satisfaction remained present.7
Since CIPII with an implantable pump is currently an invasive and costly treatment for selected patients, there is a clear need for data regarding the effects of treatment with CIPII as compared with SC insulin therapy during usual care. However, available randomised studies have a short duration (9 to 16 months) and a small number of selected participants (n = 10 to 24), and most available observational studies lack a sufficiently powered control group.8-10 In order to gain more information about glycaemic control, QoL and level of treatment satisfaction among T1DM patients treated with CIPII versus SC insulin therapy during usual care circumstances, we performed a prospective, observational case-control study.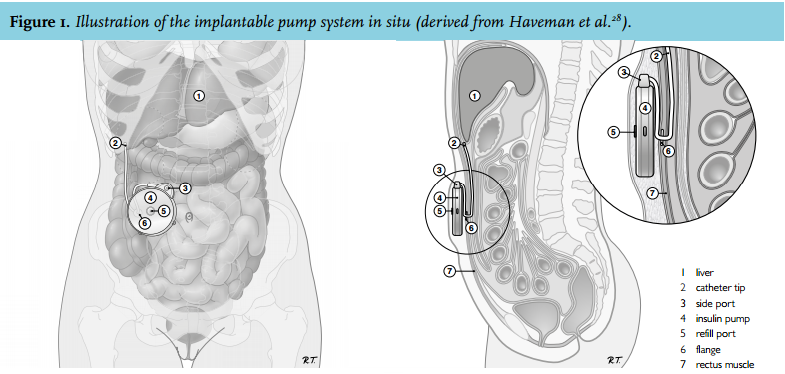
MATERIALS AND METHODS
Study design
An investigator-initiated, prospective, observational matched case-control study to compare the effects of CIPII versus SC insulin therapy on glycaemic control, QoL (including perceived health status, emotional well-being and diabetes-related QoL and diabetes-specific distress) and treatment satisfaction. The study was designed to test the hypothesis that CIPII would be non-inferior to SC insulin therapy in T1DM patients during a 26-week follow-up period. Patient recruitment took place in Isala (Zwolle, the Netherlands) and the Diaconessenhuis Hospital (Meppel, the Netherlands).
Patient selection
Cases were subjects on CIPII therapy using an implanted insulin pump (MIP 2007D, Medtronic/Minimed, Northridge, CA, USA) for the past four years without interruptions of > 30 days, in order to avoid effects related to initiating therapy. Inclusion criteria for cases to participate in this study were identical to those of a prior study in our centre and have been described in detail previously.2 In brief, patients with T1DM, aged 18 to 70 years with an HbA1c ≥ 58 mmol/mol (7.5%) or ≥ 5 incidents of hypoglycaemia glucose (< 4.0 mmol/l) per week, were eligible.
The SC control group was age and gender matched to the cases and consisted of both MDI and CSII users. Eligibility criteria for controls were T1DM, SC insulin as mode of insulin administration for the past four years without interruptions of > 30 days, HbA1c at time of matching ≥ 53 mmol/mol (7.0%) and sufficient mastery of the Dutch language.
Exclusion criteria for the present study for both cases and controls included: impaired renal function (plasma creatinine ≥ 150 µmol/l or Cockcroft-Gault ≤ 50 ml/ min), cardiac problems (unstable angina or myocardial infarction within the previous 12 months or NYHA class III or IV congestive heart failure), cognitive impairment, current or past psychiatric treatment for schizophrenia, cognitive or bipolar disorder, current use of oral corticosteroids or suffering from a condition which necessitated corticosteroid use more than once in the previous 12 months, alcohol or drug abuse, current gravidity or plans to become pregnant during the study. If patients were eligible to act as SC controls, they were matched to the CIPII-treated cases based on gender and age. The ratio of participants on the different therapies (CIPII:MDI:CSII) was 1:2:2.
Study procedures
There were four study visits. During visit 1, baseline characteristics were collected and a continuous glucose measurement (CGM) system was inserted for a period of six days. Furthermore, questionnaires were handed out and patients were asked to fill in the questionnaires concerning QoL and treatment satisfaction at home. During visit 2 (5 to 7 days later) laboratory measurements were performed, the CGM system was removed and the questionnaires were collected. During visit 3 and 4, 26 weeks after visit 1 and 5 to 7 days after visit 3, respectively, the procedures of visit 1 and 2 were repeated. During the study period all patients received usual care.
Measurements
Demographic and clinical parameters were collected using a standardised case record form. Blood pressure was measured using a blood pressure monitor (M6 comfort; OMRON Healthcare). HbA1c was measured with a Primus Ultra2 system using high-performance liquid chromatography (reference value 20-42 mmol/ mol [4.0-6.0%]). The six-day 24-hour interstitial glucose profiles were recorded using a blinded CGM device (iPro2, Medtronic, Northridge, CA, USA), inserted in the periumbilical area. Time spent in hypoglycaemia was defined as the percentage of CGM readings < 4.0 mmol/l, time in euglycaemia as the percentage of CGM readings from 4.0 to 10.0 mmol/l and time spent in hyperglycaemia as the percentage of CGM readings > 10.0 mmol/l.
Perceived health status was assessed using the 36-item Short-Form Health Survey (SF-36). Both scale and component scores (ranging from 0 to 100) were calculated.11 Emotional well-being was assessed using the World Health Organisation-Five Well-Being Index (WHO-5, range 0 to 100; higher scores indicating better QoL).12-14 Diabetes-related QoL was measured using the Diabetes-Related QoL (DQOL) questionnaire with four scales (range 0 to 100; higher scores indicating better QoL).15,16 Diabetes-specific distress was measured using the 20-item Problem Areas In Diabetes (PAID) (range 0 to 100; higher scores indicating greater emotional distress). Treatment satisfaction was measured with the Diabetes Treatment Satisfaction Questionnaire (DTSQ). Two DTSQ items assess perceived frequency of hyperglycaemia and hypoglycaemia, and six items comprise the treatment satisfaction scale (range 0-36; higher scores indicating higher satisfaction).17
Outcome measures
Since CIPII is a last-resort treatment option for T1DM, CIPII-treated patients are a highly selected population with a rather complex background and disease history. In order to account for this inequality between the two treatment groups (CIPII versus SC insulin therapy), the primary endpoint was powered based on a non-inferiority assessment of the difference in HbA1c during a 26-week period, taking possible baseline differences between groups into account. Secondary outcomes included differences in QoL, treatment satisfaction and clinical and biochemical measurements. In addition, comparisons between CIPII and patients using MDI and CSII were made.
Statistical analysis
The criteria for non-inferiority required that the upper limits of the 95% confidence intervals (CI) were above the predefined margin for the difference in HbA1c. Based on the results of previous randomised clinical trials and discussion with experts, a non-inferiority margin of -5.5 mmol/mol [-0.5%] was chosen.2-4 According to a pre-specified protocol, both per protocol and intention-totreat analysis for the primary outcome were performed. A regression model based on covariate analysis (ANCOVA) was applied in order to adjust for possible baseline imbalance in HbA1c. In the model the fixed factors CIPII and SC insulin therapy were used as determinants. The difference in scores was determined based on the β-coefficient of the particular (CIPII or SC, MDI or CSII) group. Significance of the β-coefficient was investigated with the Wald test based on a p < 0.05. The quantity of the β-coefficient, with a 95% CI, gives the difference between the two treatment modalities over the study period adjusted for baseline differences.
With the use of a standard deviation (SD) of 0.9%, estimated from a previous randomised study, and a non-inferiority margin of -5.5 mmol/mol [-0.5%], we calculated that we would need to enrol 175 patients (35 CIPII, 140 SC insulin therapy) to show non-inferiority of CIPII therapy at a one-sided alpha level of 0.025.2 In order to compensate for loss to follow-up, intended group sample sizes were 40 and 150, respectively.
Analyses were performed using SPSS (IBM SPSS Statistics for Windows, version 20.0. Armonk, NY: IBM Corp.) and STATA (Stata Corp., College Station, TX: version 12). Results were expressed as mean (SD) or median (interquartile range [IQR]) for normally distributed and non-normally distributed data, respectively. A significance level of 5% was used.
Ethical considerations
The study protocol was registered prior to the start at the appropriate local (NL41037.075.12) and international (NCT01621308) registers. The study protocol was approved by the local medical ethics committee and all patients gave informed consent.
RESULTS
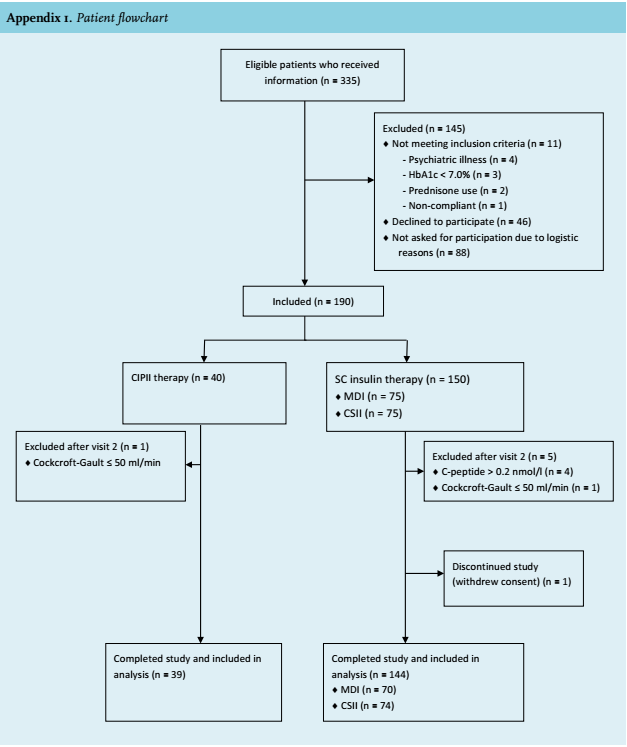
Patients From December 2012 to August 2013, a total of 335 patients were screened and received information about the study, of which 190 (57%) agreed to participate (appendix 1). After baseline laboratory measurements, two patients were excluded due to impaired renal function and four due to C-peptide concentrations of > 0.2 nmol/l. Consequently, 184 T1DM patients commenced the 26-week study period. After the first visit, one patient withdrew informed consent due to lack of interest. Therefore, 183 patients were analysed. Baseline characteristics are presented in table 1. 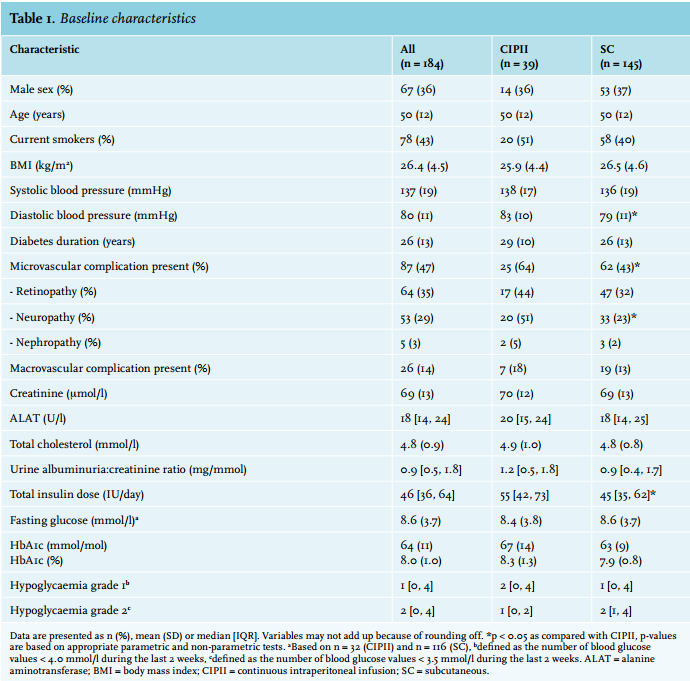
Glycaemic control
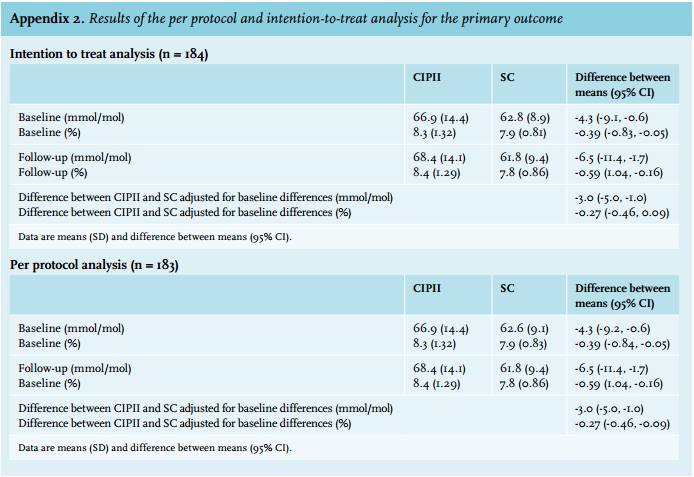
Within the group of CIPII-treated patients, HbA1c did not significantly change during the study period while it decreased by -1.0 mmol/mol (95% CI -1.9, -0.1 mmol/ mol) [-0.09%, 95% CI -0.17, -0.01] among patients using SC insulin therapy (table 2). Taking baseline differences into account, the difference between treatment groups was -3.0 mmol/mol (95% CI -5.0, -1.0 mmol/mol) [-0.27%, 95% CI -0.46, -0.09] and met the non-inferiority criterion of -5.5 mmol/mol [-0.5%]. The results of the intention-totreat analyses did not differ from the per-protocol analysis (appendix 2). The number of grade 1 hypoglycaemic episodes during the last two weeks decreased by -1.2 (95% CI -1.7, -0.7) among patients with SC insulin. Patients using SC insulin therapy spent -9.3% (95% CI -15.8, -2.8) less percentage of time in hyperglycaemia and 6.9% (95% CI 1.2, 12.5) more in euglycaemia as compared with CIPII-treated patients.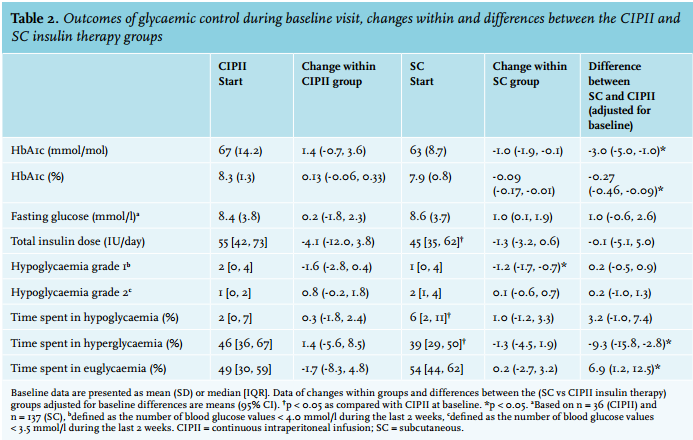
Clinical and biochemical measurements
During follow-up, a new macrovascular complication was diagnosed in three patients: one patient treated with CIPII had angina pectoris, one patient using MDI had a transient ischaemic attack and one patient using CSII had a myocardial infarction. Two patients had a new microvascular complication: nephropathy in one patient using MDI and retinopathy in one patient using CSII. Taking baseline differences into account, CIPII-treated patients had 3.6 U/l (95% CI 1.2, 6.0) lower alanineaminotransferase (ALAT) concentrations as compared with patients treated with SC insulin therapy.
Perceived health status, emotional well-being, diabetesrelated QoL, diabetes-specific distress and treatment satisfaction
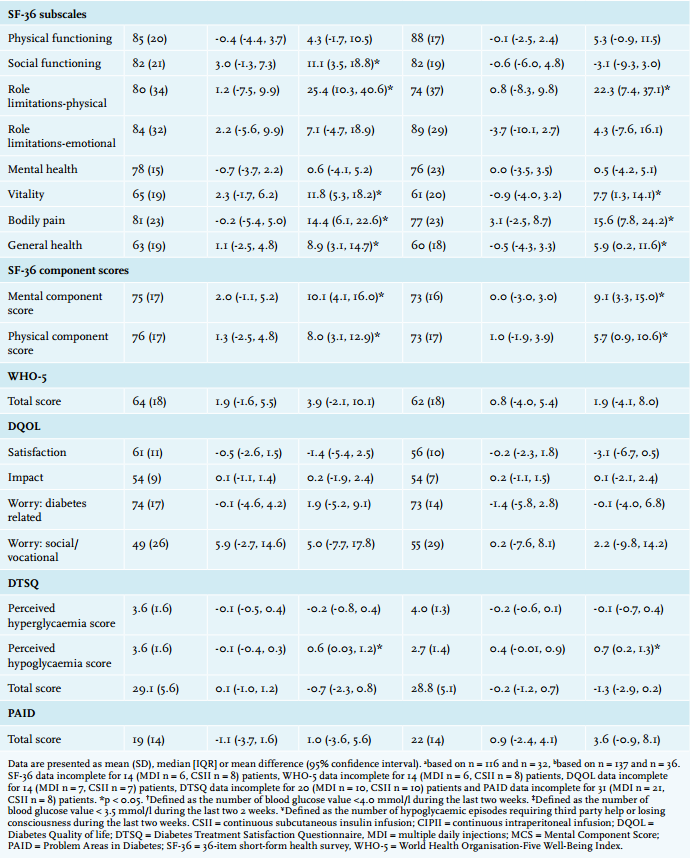
No differences within groups were observed during the study regarding perceived health status, emotional well-being, diabetes-related QoL, diabetes-specific distress and treatment satisfaction (table 3). After adjustment for baseline differences, the SF-36 subscales for social functioning, role limitations due to physical functioning, vitality, bodily pain and general health were lower among patients treated with CIPII as compared with patients treated with SC insulin. In addition, both component scores were lower. After correction for baseline differences, there were no differences in the WHO-5, DQOL and PAID scores. The percentage of patients with a WHO-5 score indicative of depression was higher among CIPII-treated patients as compared with the SC treatment group: 37% vs. 28% at visit 1 and 47% vs. 24% at visit 2 (p < 0.05 for both). Based on the DTSQ questionnaires, subjects on CIPII reported to perceive less hypoglycaemic events than subjects on SC insulin therapy: 0.7 (95% CI 0.1, 1.2).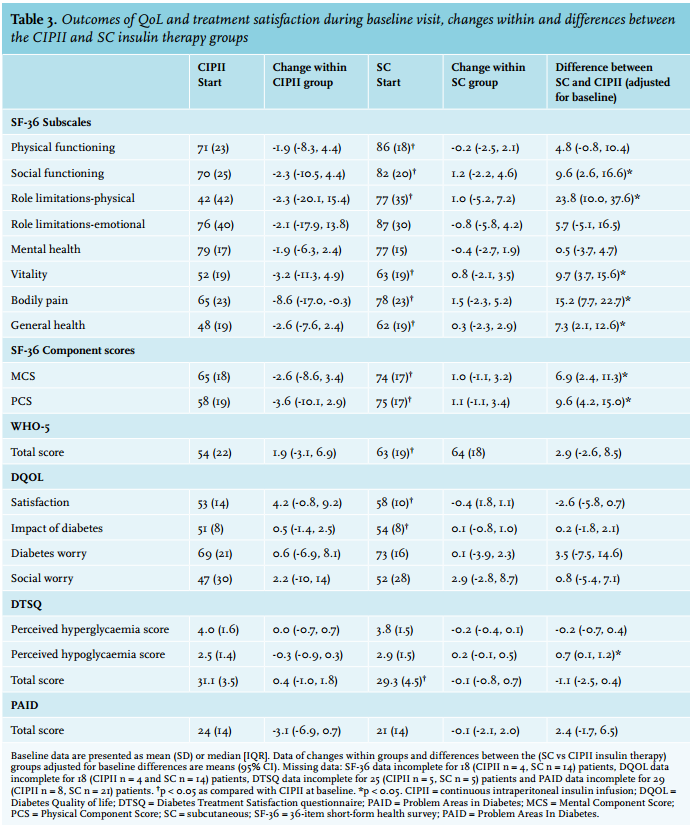
CIPII versus MDI and CSII
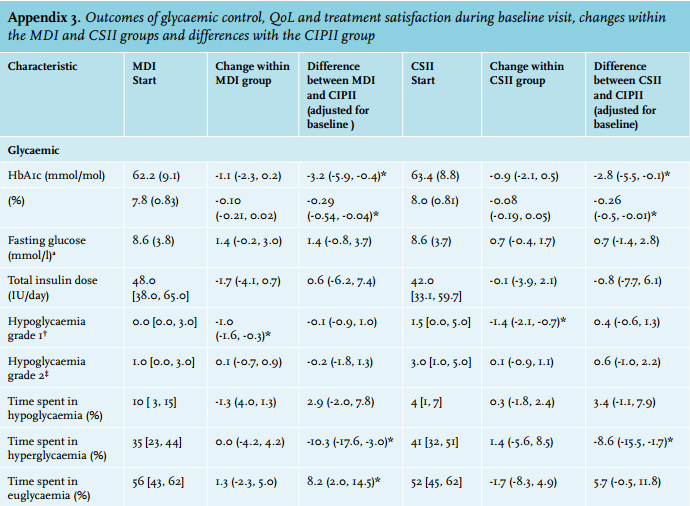
Subgroup analysis comparing patients using MDI (n = 70) and CSII (n = 74) as SC mode of insulin therapy versus CIPII-treated patients are presented in appendix 3. In comparison with the CIPII group, MDI and CSII users had a lower HbA1c (-3.2 mmol/mol, 95% CI -5.9, -0.4 mmol/ mol [-0.29%, 95% CI -0.54, -0.04] for MDI users and -2.8 mmol/mol, 95% CI -5.5, -0.1 mmol/mol [-0.26%, 95% CI -0.5, -0.01] for CSII users, respectively) and spent less time in hyperglycaemia (-10.3%, (95% CI -17.6, -3.0) for MDI users and -8.6% (95% CI -15.5, -1.7) for CSII users, respectively) after adjustment for baseline differences. In addition, MDI users spent 8.2% (95% CI 2.0, 14.5) more time in the euglycaemic range than CIPII-treated patients. Perceived health status scores were lower for CIPII-treated patients as compared with both MDI and CSII users. In addition, CIPII-treated patients had a lower score on the perceived hypoglycaemia score, as compared with both MDI and CSII users.
DISCUSSION
The aim of the present study was to compare glycaemic control and QoL data from T1DM patients treated with long-term CIPII therapy relative to a control group of patients treated with SC insulin therapy during usual care. According to the study protocol, the HbA1c difference between the two treatment groups was assessed using a non-inferiority method. Although the HbA1c difference of -3.0 mmol/mol (95% CI -5.0, -1.0) [-0.27%, 95% CI -0.46, -0.09] between the groups was negative, implying a lower HbA1c for subcutaneously treated patients, the 95% CI remained above the predefined margin of -5.5 mmol/mol [-0.5%]. Therefore, it should be concluded that CIPII is non-inferior to SC insulin therapy with respect to HbA1c in the treatment of T1DM during usual care circumstances. The effects of CIPII versus SC insulin therapy on glycaemia have been described previously in three randomised studies. After six months of cross-over treatment with CIPII and SC insulin, Haardt et al. reported a difference of 14 mmol/mol [1.28%] in favour of CIPII, with a reduction of glycaemic fluctuations and hypoglycaemic episodes.4 A previous cross-over study in our centre among 24 T1DM patients found an HbA1c decrease of 8 mmol/mol [0.76%], with 11% more time spent in euglycaemia without a change in hypoglycaemic events, in favour of CIPII.2 Subsequent observational studies among CIPII-treated patients found stabilisation of the HbA1c during long-term follow-up at an equal or lower level than before initiation of CIPII.7-9,18 The results of the present study extend the literature by providing a sufficiently powered assessment of the glycaemic status during real-life circumstances among T1DM patients treated long-term with CIPII, relative to a SC insulin therapy control group. Although the difference in HbA1c was non-inferior, it should be noted that patients treated with CIPII had a higher glycaemic profile compared with patients treated with SC insulin therapy.
During the aforementioned cross-over study in our centre, perceived health status and general QoL improved during six months of CIPII as compared with SC insulin therapy.6 During the subsequent six years of follow-up, the perceived health status among these CIPII-treated patients was stable.7 The present study adds to these observations by demonstrating that the perceived health status among patients treated with CIPII is stable, but remains poor as compared with matched subjects treated with SC insulin therapy. In contrast to the perceived health status, we found no differences in general and diabetes-related aspects of QoL and the total treatment satisfaction scores between CIPII and SC insulin therapy, after adjustment for baseline differences. This discrepancy may suggest that, although the presence of microvascular complications may be of influence, the poorly perceived health status among these patients is not due to their diabetes per se but that probably other factors also have an important influence. Possible factors may include poor social functioning, limited support or more (perceived) physical limitations and pain. Additionally, the presence of the personality traits and psychiatric symptoms, identified previously by De Vries et al. and emphasised in the present study by the high number of CIPII patients with a WHO-5 score indicative for depression, may explain this discrepancy.19
The presence of frequent hypoglycaemic episodes (often combined with hypoglycaemia unawareness) is an indication for initiation of CIPII and intraperitoneal insulin administration results in more predictable glucose profiles and a restoration of the hepatic response to hypoglycaemia. A reduction in perceived hypoglycaemia threat may, therefore, be an important determinant of diabetes-related QoL and treatment satisfaction among CIPII-treated patients.20-22 This is also reflected by the hyperglycaemic profiles and lower perceived hypoglycaemia score even though there was no actual decrease in the number of self-reported hypoglycaemic events among CIPII-treated subjects. In addition to a lower frequency of hypoglycaemic episodes, a reduction in the number of days spent in hospital during CIPII therapy has been suggested to have a positive influence on diabetes-related QoL and treatment satisfaction.2,7,19
Besides lower ALAT concentrations among CIPII-treated patients, there were no other differences in clinical and biochemical parameters between groups. Although ALAT concentrations were still within the normal range and the other liver enzymes were stable, this finding is remarkable. It might be hypothesised that, since intraperitoneal insulin administration results in higher hepatic insulin concentrations than SC insulin, this leads to altered hepatic metabolism secondary to higher insulinisation.23-25
This is the first study to compare the effects of CIPII and SC insulin administration in a large population of poorly regulated T1DM patients receiving usual care during real-life circumstances. The non-randomised design remains the major limitation of the present study. However, the complexity of the CIPII-treated group necessitated pragmatic measures in the study design. Although patients were on the same therapy for more than four years, measurements were performed with a 26-week interval, outcomes were adjusted for baseline differences and groups were well matched on age, gender, HbA1c and hypoglycaemic episodes at baseline, differences between groups that are known to influence glycaemic control could still be present.26,5 Although hypothetical, the presence of such unmeasured differences between groups may have caused a slight underestimation of the effect of CIPII on glycaemic control. While fully acknowledging these limitations, we feel that the current design is the best available for the present study objective given the real-life, clinical restrictions.
At present, the costs of CIPII, estimated to be approximately € 6000 higher on an annual basis than CSII, seem to outweigh the advantages of CIPII for the majority of patients and health care systems.27 Nevertheless, based on the short-term positive effects found in previous studies, including HbA1c improvements, less hypoglycaemic episodes and improved QoL, and the findings of the present study among CIPII-treated patients relative to SC insulin therapy during usual care, we advocate that CIPII using an implantable pump should still be seen as a feasible last-resort treatment option for selected patients with T1DM who are unable to reach glycaemic control with SC insulin therapy.2,4,7,5
ACKNOWLEDGMENTS
The authors would like to thank all internists and diabetes specialist nurses from the Isala and Diaconessenhuis hospitals for their help in conducting the study. Furthermore, we would like to thank Medtronic and Bayer for their support in providing the CGM devices and blood glucose meters.
DISCLOSURES
The authors have no financial or other relationships that might lead to a conflict of interest.
PRvD is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The iPro2 glucose monitoring systems and Enlite sensors for the continuous glucose measurements were sponsored by Medtronic International Trading Sarl (Switzerland). The Contour XT blood glucose meters were sponsored by Bayer Diabetes. Neither of the sponsors had a role in the study design, data collection, analysis, interpretation, or in the writing the report.
REFERENCES